
Abstract
COVID-19 has posed a considerable threat to all aspects of older Americans’ lives. The pandemic generated acute illness, emergency department (ED) visits, hospitalization, respiratory failure, and death. Pandemic-associated social isolation and loneliness further endangered older adults. Recovery from COVID-19 illness has commonly been followed by chronic symptoms, which may also precipitate ED visits. While vaccination has mitigated risks of serious illness requiring hospitalization, a booster dose is required to sustain protection. New treatments and therapies, including monoclonal antibodies and antiviral agents, have shown efficacy for older adults who are at risk of hospitalization. Older adults remain vulnerable in 2022, after two years of the COVID-19 pandemic. Emergency care for older patients is now challenged with health system staffing shortages and diminished access to care in community programs & skilled nursing facilities. This article attempts to synthesize the avalanche of discovery and innovation into a narrative review focused on the emergency and immediate post- ED care of the aging adult patients both during and as a result of the COVID-19 pandemic.
Box 1: Patient Scenario 1
An Older Patient Presents to the ED for Treatment
A 79-year-old Laotian woman who lives in the community with her family was seen by her primary care provider at a routine follow-up visit in early January 2022. She was noted to have a cough with congestion. She had no loss of smell and no gastrointestinal symptoms. She had no known sick contacts.
Past Medical History: Diabetes mellitus, osteoarthritis, peripheral neuropathy, depression, osteopenia, subclinical hypothyroidism, and hypertension. She received a COVID vaccination (Feb and March 2021) but did not get a booster dose. She needed assistance for bathing but otherwise was independent in her self- cares.
Medications include: lisinopril 5 mg daily, metformin XR 500 mg daily, vitamin D 2,000 units daily, atorvastatin 20 mg daily, meclizine 12.5 mg daily prn, and gabapentin 100 mg each night. BP 173/96. Pulse 89/ minute. Pulse ox=97% on room air. Respiratory rate= 20 per minute. Temperature= 98.6. BMI= 25. Physical examination was remarkable for normal attention and level of consciousness. Her cardio-pulmonary examination was normal. Her COVID-19 test in the primary care office was positive.
- Which medication or treatment could be considered?
- How would you counsel the patient regarding her co-morbid illnesses?
Box 2: Patient Scenario 2
An Older Patient Presents to the ED with a Cascade of Symptoms and Functional Decline after COVID-19
A 73-year-old community-dwelling woman was brought to the ED by her daughter who reports that the patient had a decline in function and cognition after her recent hospital discharge. Her daughter reports having trouble managing her at home. The patient was noted to be sleeping all day, and not eating. She was generally weak and complained of pain in both of her legs. She missed her most recent dialysis, as she was too tired. She required two family members to assist with transfers. Prior to her hospitalization, she required only one person to assist.
Fourteen days ago, her family brought her to the ED 3 days after testing positive for COVID-19. She received no vaccination for COVID-19. At that time, her symptoms included a runny nose, cough productive of green sputum, and nausea. There was no hypoxia. She had missed dialysis once due to difficulty coordinating care with active COVID-19 infection. Her initial admission labs were significant for hypokalemia and hyponatremia. Physical therapy and occupational therapy noted a decline from her baseline function. Her recent hospital length of stay was 3 days.
Past Medical History: Multiple co-morbidities included ESRD (receiving dialysis on T/Th/S), dementia, cerebrovascular accident, atrial fibrillation, coronary artery disease with NSTEMI in 2020, hypertension, osteoarthritis, and protein calorie malnutrition. Her multiple medications included apixaban.
Social history was notable for the daughter being her paid personal care provider.
The ED was overcrowded with 20 boarding admitted patients.
- What are common problems for older patients with recent COVID-19 infections?
- How would you determine the best strategy to help this older patient and her family caregivers?
- How do we access community and long-term services to support this patient and family caregiver?
Background
During the last two years of the COVID-19 pandemic, the emergency department (ED) has been the interface between our community and our health care system. As of March 13, 2022, over 79.5 million cases and 967,711 deaths have been attributed to COVID-19 in the United States (US).1 This paper will provide key points about COVID-19 in older adults for emergency medicine providers, as exemplified in the case scenarios (Boxes 1 and 2). We will present a succinct review of COVID-19 epidemiology in older adults and review the presentation of both acute illness and the sequelae of COVID-19 illness. We will review reports of vaccination protection in older adults, ED treatment strategies, and the implications of COVID-19 on systems of care affecting older patients. Finally, we will describe the impact of the pandemic on the ED workforce.
Epidemiology
Age is associated with severe COVID-19 outcomes. More than 54.1 million people are aged ≥ 65 years in the US. In 2020 these older persons suffered 81% of U.S. COVID-19 related deaths, and as of September 2021, their mortality was over 80 times greater than those aged 18-29 years.2,3 Although residents in long-term care facilities made up < 1% of the U.S. population, those residents suffered 16% of all COVID-19 deaths.4-8 Additionally, the COVID-19 mortality risk and disease severity associated with any high-risk condition increases with age.9,10Lastly, older adults infected with COVID-19 were more likely than younger adults to require hospitalization, develop pulmonary failure, and need either noninvasive or invasive ventilation.11
Acute Presentation of COVID-19 in Older Adults
COVID-19 is a multi-organ disease and therefore causes a broad spectrum of signs and symptoms.12 COVID-19 patients typically exhibit nonspecific symptoms of both upper and lower respiratory infection along with occasional nausea, vomiting, and diarrhea. One population screening study of 1,279 people demonstrated that fever, ageusia (loss of sense of taste), and weakness increased the odds of infection, while 36% of people testing positive were asymptomatic.13
In a Cochrane review of 44 studies, including 10 from the ED, only cough and fever had a sensitivity of at least 50% for COVID-19 illness.14 These studies used a positive RT-PCR as the reference standard, as well as clinical expertise and imaging. The presence of anosmia (loss of sense of smell) or ageusia had sensitivities below 50% but, specificities of 93%. However, the majority of signs and symptoms heralding potential COVID-19 infection had very poor diagnostic accuracy. Neither the presence nor absence of commonly attributed COVID-19 symptoms were accurate enough to be predicative or capable of excluding active illness. However, simple fever and cough may be useful to identify people for further testing, and the presence of anosmia or ageusia can serve as “red flags” for acute illness. There is a paucity of solid evidence for diagnosis of COVID-19 in older adults. COVID-19 signs and symptoms along with most serious infections in this population such as bacterial pneumonia, and urinary sepsis, all lead to non-specific presentations. The older adult’s presenting signs and symptoms can be used with diagnostic testing during the acute presentation in the ED. Notably, however, a negative RT-PCR test does not rule out COVID-19 and should not be used as the sole basis for treatment or management decisions. A false negative test could occur if testing was performed too early or too late to make an accurate diagnosis with the RT-PCR.15
The categorization of potential illness into actionable groups based on illness severity is more impactful to the emergency clinician.16,17 Mild or moderate illness symptoms include fever, cough, aches, and lethargy without dyspnea at rest. Severe symptoms include dyspnea, tachypnea, and hypoxia, with features ranging from pneumonia to acute respiratory distress syndrome (ARDS), shock, or other organ dysfunctions. Kennedy and colleagues documented that delirium often existed without any other typical signs or symptoms of COVID-19 infection.18 Delirium was also associated with poor hospital outcomes and death. Delirium should therefore be considered as an indication for screening, testing, and evaluation for COVID-19 infection in older adults.
Long-Haul Presentation of COVID-19 in Older Adults
Descriptions of post-acute sequelae lasting beyond 12 weeks have been termed post-COVID-19 syndrome or long-haul COVID.19 Long-haul COVID incidence is predictably rising following high rates of omicron infection. Easy fatigability is the most common symptom of this COVID-19 complication. One study noted fatigability in 51% of those with long COVID findings. Anxiety, dyspnea, and headache were each noted in 38%.20 Most studies followed a cohort of patients 60 days after their diagnosis, symptom onset, or hospitalization; or for 30 days after their recovery or hospital discharge. Studies typically use surveys imaging and/ or diagnostic clinical assessments outside of the ED.21 ED physicians and nurses should be aware that in some patients, symptoms may persist long after recovery from COVID-19. To make the diagnosis of long haul COVID-19 in older adults in the ED, the clinician would need to assess for a functional decline during the COVID-19 illness or find an acute illness that could explain the symptoms.
In one bit of favorable news for older adults, they are less likely than the younger cohort to experience post- COVID psychological distress such as PTSD, depression, and anxiety.22 Older adults generally exhibit higher levels of resilience to pandemic-related psychological stress.23,24 In cognitively intact older adults, age may buffer COVID-19 related mental health deterioration.25 Yet the harms of social isolation were not examined in these studies.
Older adults demonstrate higher rates of cognitive difficulties, persisting for months after discharge from COVID-19 hospitalization.26 New onset dementia has been noted in about 2% of patients over age 65 in the first 14-90 days post- COVID-19 diagnosis.27 This new dementia may cause increased ED presentations and require increased home supports to allow ED discharge. Enhanced access to cognitive screening from the ED should be considered for older adult COVID-19 survivors. Further research of long-haul COVID-19 will need to be integrated into ongoing research on ED dementia care.28
Treatments and Management in the ED
Therapy
The use of ethical principles such as maximizing benefit to the greatest number, preventing harm, and mitigating health inequities, may allow ED prioritization for access to new therapies with limited availability.29 Shared decision-making in the ED is fundamental during the care of older adults.30,31 ED providers have learned from pandemic resource shortages that the time to develop these strategies is before the next wave of illness outpaces resources.32
The ED management of COVID-19, as with all illnesses, focuses first on stabilization of life threats. In COVID-19, the first and most important mainstay of treatment is supplemental oxygen. Supplemental oxygen can render patients eupneic, greatly reducing the potential for respiratory exhaustion.33 Advanced age is associated with a high risk of pulmonary failure, need for mechanical ventilation, and death. Age ≥ 85 years, dyspnea, and polypharmacy are important predictors of mortality.34 The amount of supplemental oxygen reaching the alveoli maximizes at a FiO2 of 44%, with flows in excess of 6L.35 FiO2 can be increased to 100% when used with a 10 -15L/min flow rate.36 Oxygen delivery may be further increased by high flow nasal cannula (HFNC) devices, which maintain FiO2 at 100% while increasing flow to as much as 60L/min.37 The use of high-flow oxygen through a nasal cannula significantly decreased the need for mechanical ventilation support and time to clinical recovery compared with conventional low-flow oxygen use.41, 42
If patients remain hypoxemic despite maximal therapy with HFNC, they are typically placed on higher levels of support such as CPAP or invasive mechanical ventilation (IMV). One study showed HFNC use effectively prevented IMV in 71.4% of patients.38 Another study showed that one-third of hypoxic COVID-19 patients on HFNC did not require intubation.39 Cochrane review determined that HFNC likely improves treatment compared to standard oxygen but makes little or no difference to treatment failure compared to NIV or NIPPV. Comfort is of particular importance in tolerating any therapy in cognitively impaired individuals. It is important that improvement in either short-term or long-term comfort with HFNC proved of very low certainty.40 Among patients with severe COVID-19, HFNC seems to be an effective and safe treatment modality in acute respiratory failure.
Vaccination
A paucity of older individuals was studied in published and ongoing phase II-III clinical trials evaluating COVID-19 vaccine efficacy. We know older people suffered the highest consequences of morbidity and mortality from COVID-19. They were also the first population to be vaccinated. This resulted in a large population available for a vaccine efficacy study. However, only 9.83% of any study participants were ≥ 65 years, 1.66% ≥ 75 years, and < 1% were ≥ 85 years.43 Also striking is the lack of studies supporting the efficacy and safety of COVID-19 vaccines on older persons with frailty, disability, or living in long-term care facilities.44 A recent study examined the immunogenicity and adverse reactions of BNT162b2 mRNA vaccines in older adults with frailty or living in long-term care facilities. The vaccine produced immunogenicity, independent of age, or level of frailty and co-morbidity. The small sample size and inclusion criteria are cause, however, for further study.45
As of March 13, 2022, 91.3% of adults aged 65 to 74 years and 85.6% of adults age ≥ 75 years are fully vaccinated for COVID-19.46 The immunization of older people with either mRNA or vector-based vaccines decreased the likelihood of severe cases needing ICU care by more than 90%.47 In adults ≥ 50 years two doses of mRNA vaccine demonstrated 89% effectiveness against laboratory confirmed infection requiring hospitalization, 90% effectiveness against ICU admission, and 91% effectiveness regarding ED or urgent care clinic visit. Two vaccine doses provided protection in persons ≥ 85 years varying from 81- 95% for hospitalization, ED, or urgent care clinic visits. Given the concern for impaired immune response with aging these data are encouraging.48 Vaccinations did not entirely prevent post-vaccination COVID-19 infections, termed breakthrough infections. Seventy percent of breakthrough infections requiring hospitalization occurred in adults ≥ 65 years. Older persons also accounted for 87% of breakthrough mortality.49 However, the majority of breakthrough infections in post-vaccinated patients were mild or asymptomatic.50
Boosters
In older patients, the risk of COVID-19 illness increases six months after the initial vaccination. Decreased protection against hospitalization and death was greater in those ≥ 65 years at 20 weeks or more after vaccination. Greater waning of effectiveness against hospitalization was noted with the delta variant and with the increase of clinical vulnerability.
However, booster vaccination rapidly induces a recurrent and robust immune response. This was found across all ages, with older adults defined as age ≥ 60 years of age.51-54 The administration of a third COVID-19 mRNA vaccine dose improved protection against COVID-19 associated hospitalization.55 Omicron variant infection outcomes were also improved by booster vaccination doses. As of January 8, 2022, infection incidence and hospitalization, and mortality rates were lowest in those having booster doses.56 People receiving a booster at least 5 months after a second vaccine dose had 90% lower COVID-19 mortality.57 Rates of severe illness were lower in the ages ≥ 60 years booster group, by a factor of 21.7%.51
Importantly, longer intervals between doses provided higher serologic responses and increased vaccine effectiveness.58 An optimal dosage interval has yet to be reported. Heterologous boosting is defined as the administration of the booster dose from a different manufacturer than was given in the primary series. Heterologous vaccination in all adults, including those > 61 years, resulted in more robust immune responses than homologous boosting and might enhance protection.59
On March 15, 2022, Pfizer and BioNTech sought authorization from the Food and Drug Administration for a second COVID-19 booster shot for older Americans 60
Several strategies have been suggested to enhance vaccination acceptance in older adults. The Society of Academic Emergency Medicine presents resources for overcoming barriers to vaccination.17 Additionally, healthcare workers can enhance vaccination in this population by the incorporation of known communication strategies, questions, and prompts.61 Novel vaccine platforms and adjuvant systems should be considered to enhance the vaccination in older adult populations.62 We encourage ED systems to routinely offer COVID vaccination, especially since EDs routinely provide vaccination for illnesses of far less public health impact, such as tetanus.17 The offer of a vaccine for respiratory transmissible infection may have greater acceptance in patients presenting to the ED with concern, but testing negative for, the illnesses of influenza or COVID. Lastly, a global strategy enhancing older adult immunization as part of a public health agenda could decrease the suffering for the billions of older persons at risk of death and disability from vaccine-preventable diseases.63
Treatment Resources for ED Providers
Therapies for the treatment of COVID-19 are still in development with no effective curative therapy yet available. Table 1 describes COVID-19 treatment and resources for older adults.17, 64-70 Most of the guidelines and websites describe evidence-based care, without overtly defining older adult considerations. The Infectious Disease Society of America site,65 and the WHO site,68 note specific older adult considerations. The geriatrics portion of the American College of Emergency Physicians COVID-19 Management tool, 64 provides information from the early pandemic. The Society of Academic Emergency COVID Provider Toolkit, 17 provides succinct communication strategies, as well as interactive treatment recommendations. Finally, a side-by-side tool from the Health and Human Services is a clinician-friendly, graphic depiction of considerations for prescribing and administering treatments for those with mild to moderate COVID-19.70
Table 1: COVID-19 Treatment and Resources for Older Adults
Links from Table 1: COVID-19 Treatment and Resources for Older Adults
ACEP COVID-19 Field Guide64
Date updated: July 13, 2021 Geriatrics section from early in the pandemic.
Geriatric EM Centeredness: One chapter in this resource was specific to older adults-social isolation; inter-facility transfers.
Components of the Resource: General descriptions of presentation of illness and systems-based ED strategies early during the first wave of the pandemic
Infectious Disease Society of America Real-Time Learning65
Date updated: March 8, 2022 Geriatrics section updated November 9, 2021.
Geriatric EM Centeredness: Geriatrics was included within patient populations. Key areas included delirium, frailty, dementia, and clinical features plus resources.
Components of the Resource: Table and clear outline helped to synthesize the treatments, the setting of care, the recommendations, and the certainty of evidence.
NIH COVID-19 Treatment Guidelines 66
Date updated: March 2, 2022
Geriatric EM Centeredness: The approach for older adults was integrated into the guidelines, but not defined in special populations. A succinct description was provided on follow-up after ED care.
Components of the Resource: A detailed website with guidelines in the context of care. The summary of recommendations was helpful. Ratings of evidence and ratings of recommendations were provided.
The European Society of Clinical Microbiology and Infectious Diseases COVID19 Living Guidelines67
Date updated: February 1, 2022
Geriatric EM Centeredness: No specific recommendations for older adults in special populations. The approach to older adults was not integrated into the guidelines.
Components of the Resource: Regularly updated guidelines with detailed data tables which provide a synthesis of evidence. Clinical questions focused on population, intervention, comparison, and outcomes (PICO). Difficult to navigate the resource tables.
WHO Living COVID-19 Guideline68
Date updated: November 23, 2021
Geriatric EM Centeredness: A thoughtful and succinct area of this guideline described practical considerations for assessment and care of older adults with COVID-19.
Components of the Resource: Well-written synthesis of evidence with easy-to-navigate pdf and website. Recommendations for clinical management scenarios.
US Federal Response to COVID-19 Therapeutics69
Date updated: February 15, 2022
Geriatric EM Centeredness: No specific description of the unique needs of older adults, beyond renal disease and drug-drug interactions for Paxlovid.
Components of the Resource: This resource focuses on the mild to moderate COVID-19 in high-risk patients. Includes a graphic summary of the setting of care with treatment considerations.
Health and Human Services Side by Side Overview of COVID-19 Therapeutics70
Date updated: March 1, 2022
Geriatric EM Centeredness: Geriatrics considerations are noted, including adjustment for renal impairment, drug-drug interactions, and Medicare coverage.
Components of the Resource: A quick reference for outpatient therapies for prevention of COVID19 infection or treatment of mild to moderate COVID-19. The simplicity of the tool allows for details of how to prescribe each treatment/ medication.
Society of Academic Emergency Medicine COVID19 Provider Toolkit17
Date updated: January 3, 2022
Geriatric EM Centeredness: Strategies to improve communication with older adults are integrated into the materials. Treatment recommendations are not specific for older adults.
Components of the Resource: This interactive website provides (evidence-based) succinct treatment recommendations as well as strategies to improve communication with patients who have COVID-19.
Monoclonal Antibody (mAb) Treatments
Monoclonal antibody (mAb) treatment is associated with decreased hospitalization and death in outpatients with mild to moderate COVID-19.71-74 Older age is an indication for mAb treatments 70 These treatments are especially important for ED providers discharging patients home with mild to moderate COVID-19 symptoms. We will not describe the mAb treatments which are not likely to be active against the omicron variant and limit our focus to sotrovimab.
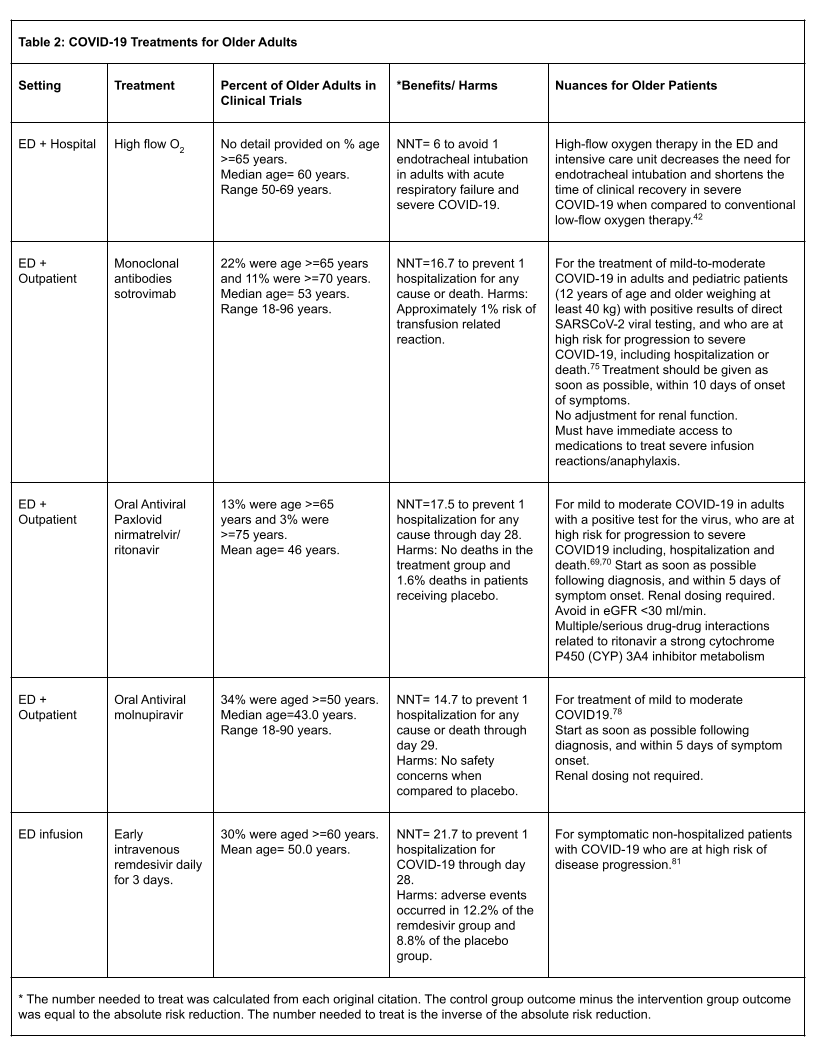
- Sotrovimab treatment has resulted in a 79- 85% reduction in hospitalization or death in high-risk adult outpatients compared to placebo.75 This drug has activity against the Delta variant and is likely active in the Omicron variant.68 Sotrovimab, similarly to the other mAb treatments, is authorized only for the treatment of lab-confirmed mild to moderate disease within ten days of symptom onset. See Table 2.
- Monoclonal antibody treatments are an effective treatment for those with laboratory-confirmed COVID-19 who are ≥ 65 years. Additionally, they may be used for younger patients at high risk of progressing to severe illness 70 See important details that refer to eligible populations. These treatments are NOT authorized for hospitalized patients nor for those who require oxygen therapy. Recommendations for monoclonal antibody medication are often made at a regional/local level, based on the treatment that best covers local variants
Therapy with monoclonal antibodies changes rapidly subject to the latest available evidence and guidance of the Center for Disease Control. These therapeutics are distributed via the HHS Office of the Assistant Secretary for Preparedness and Response transitioned to a State and Territory-coordinated Distribution System for mAbs.76
Oral Antivirals
- Paxlovid has shown an 88% reduction of hospitalization or death for high-risk patients if given within 5 days of symptom onset.69,70 It has known activity in the Delta variant and data is pending on Omicron variant activity. Table 2 highlights the high risk of drug-drug interactions and comorbid illnesses which is relevant to older adults. The percentage of older adults in the clinical trial was low.
- Molnupiravir has shown a 30% reduction of hospitalization and death for high-risk patients if given within 3 days of symptom onset. It has known activity in the Delta variant and data is pending on Omicron variant activity.77 In a phase 3 trial of 1,433 persons who were unvaccinated with mild to moderate laboratory-confirmed COVID illness and at least one high risk factor for severe disease, molnupiravir reduced the risk of hospitalization or death when started within 5 days of symptoms.78 The effectiveness of molnupiravir is competitive to the three monoclonal antibodies remdesivir and nirmatrelvir-ritonavir, with a relatively lower cost.79 An FDA expert panel review showed that molnupiravir with 50% hospitalization reduction was inferior to the three existing monoclonal antibody cocktails having over 60% efficacy. However oral availability and decreased expense of molnupiravir lead to ultimate approval recommendation.80 Table 2 highlights the low rate of older adults in the clinical trial of this medication.
Other Treatments
- Remdesivir has mixed data on efficacy against COVID disease progression. One study shows that a 3-day course resulted in 30% of patients > 60 years with 87% lower hospitalization risk or death, and an acceptable safety profile.81 Please see Table 2. Another trial concluded that remdesivir shortened the time to recovery in hospitalized patients with lower respiratory tract infections. 82 However, a Cochrane review found moderate certainty that remdesivir has little or no effect on all-cause mortality at up to day 28 in hospitalized adults with SARS-CoV-2 infection. 83 Finally, one study showed an association with longer hospital stays.84
- Convalescent Plasma (CP) some studies demonstrated that early administration of high-titer CP reduced the progression of COVID-19 in mildly ill older adults.85 An October 2020 Cochrane review update detailed the uncertainty of the benefit of CP treatment.86 Finally, a December 2021 scoping review included 154 studies- with 112 studies concluding CP is safe and resulted in clinical improvement.87
- Steroids, in patients hospitalized with COVID-19, the use of 6 mg daily of dexamethasone resulted in lower 28-day mortality among those who were receiving either invasive mechanical ventilation or supplementary oxygen, but not among those who did not need respiratory support.88 In the RECOVERY study no benefit of the use of steroids was observed in patients of older age or higher number of co-morbidities.89 The use of dexamethasone resulted in a 30% reduction in 28-day mortality among patients receiving invasive mechanical ventilation compared to the usual care group. No benefit was found among patients not requiring respiratory support. The WHO strongly recommends corticosteroids (i.e., dexamethasone, hydrocortisone, or prednisone) for the treatment of patients with severe and critical COVID-19.68
Psycho-Social Implications for Older Adults During the Pandemic
Social isolation and loneliness have been important health challenges for older adults during the COVID-19 pandemic.90, 91 Social isolation and loneliness are major risk factors linked with poor physical and mental health status. Mandates for stay at home and social distancing have exacerbated social isolation and loneliness. Economic insecurity, difficulty accessing health care services, and racial inequities compound the situation. Some innovative voice-controlled intelligent technologies have been implemented to counteract COVID- era loneliness.92 Emergency medicine physicians seldom recognize social isolation and its detrimental impact on the daily lives of vulnerable older adults.93
Many older adults presenting to the ED may not have left home or had any interaction with a medical provider for weeks to months. The ED is often the site where family caregivers turn when they are unable to care for their loved ones. Efforts to identify medical problems are improved by an assessment of the individuals’ social supports and their access to community resources. Knowledge of these supports is critical for safe discharge in this population.
If the ED assessment shows that the patient does not require admission to the hospital, it is imperative providers understand the availability of current community resources. The pandemic has limited available usual resources, especially personnel. Typical orders for home care or other support services may not be available. A shortage of resources is a common theme. Community programs may be in short supply, including non-medical home care, transportation, community meal sites, behavioral health programs, in-person counseling, and aging services from the county to support family caregivers. Skilled home care agencies have, likewise, faced an increase in referrals with a lack of staff to provide the services. Table 3 shows how ED physicians can access community resources for older adults. Knowing and acting on what matters most to the older person honors the individual’s choices. 94
Caring for Individuals with Alzheimer’s Disease or Related Dementias
The number of older adults in the U.S. living with dementia or related disorders has increased with continued rise projected in the coming decades.95, 96 Therefore, ED teams are increasingly more likely to evaluate and treat individuals living with dementia.97
Individuals living with cognitive challenges often experience negative effects from busy ED environments. Loud noises, bright lights, overcrowding, and long waits to be seen, admitted, or discharged may all contribute to sensory overload and increased anxiety. In addition, building rapport quickly with unfamiliar providers may be difficult for individuals with mild, moderate, or advanced dementia.98 These challenges have precipitated the need to improve dementia care in the ED and the evidence base on which to provide that care. GEAR 2.0 ADC provides recommendations for screening, communication, best care practices, and care transitions.28
COVID-19, isolation, and limited social interactions have contributed to reduced physical activity, depression, and loneliness among older adults and care partners.99, 100 Limited physical activity and social isolation also contribute to accelerated cognitive decline. 101 As a result, family stress levels are heightened. Care partner capacity often influences whether or not a person living with dementia is taken to the ED or if they can return to their home or community safely.102
The challenges of living with an older adult who is experiencing symptoms related to dementia have increased, and many care partners accompanying a person with dementia to the ED show signs and symptoms of weariness, anxiety, and exhaustion. In some cases, family or other care partners become ill themselves or are unable to find a paid caregiver due to the current staffing crisis.103
Unfortunately, while many low or no-cost programs and services exist in most communities, ED staff members may not be aware of them, or may not have resources to make helpful referrals to support families.104, 105 An interprofessional team approach has been effective106 where social workers or care managers assist in providing information on community resources and follow up with primary care providers and/or dementia specialists. Reduced social worker or care manager hours in the ED limits patient or care partner access to the individuals on the team who are most familiar with community services such as Area Agencies on Aging (AAAs), senior centers, nutrition programs, home care agencies, and others. Table 3 provides online search tools for local community resources for older patients and their family caregivers.
Table 3: Community Resources to Safely Assist Older Adult Returning Home from the Emergency Department
Links from Table 3: Community Resources to Safely Assist Older Adult Returning Home from the Emergency Department
Eldercare Locator
Services: Housing, transportation, services, and support services
Description: This user-friendly website from the U.S. Administration on Aging provides a link to local community resources based on the individual’s zip code.
Older Veterans Services
Services: Veterans Health Care for Elderly Veterans. Pension information.
Description: This website provides links to Veterans Affairs benefits and services with searchable resources based on the Veteran’s zip code.
Alzheimer’s Association
Services: Caregiver support groups, counseling, and 24/7 Helpline.
Description: This website provides resources to support family caregivers of individuals who have Alzheimer’s disease and related dementias
Find Help.org
Services: Community-based organizations and resources for food, housing, transportation, etc.
Description: A free online tool to find social services by zip code. Developed by auntbertha.com.
Challenges for Residential Care Centers and Implications for Transitions
Recruiting and retaining qualified staff, particularly clinical staff providing hands-on care, has been a challenge in nursing facilities and assisted living facilities for many years. High rates of staffing turnover in positions of nurses and nurse aides, are well documented and have been correlated with quality concerns, including citations related to infection control.107 A recent article found that the average annual turnover rate for total nursing staff in these facilities was 128%.108 Now, the situation is even more critical.109 As in many healthcare settings, burnout has led to clinical staff leaving the front lines. In addition, nursing facilities are competing with hospitals and staffing agencies that are offering significant financial incentives. While most nursing facility staff have received the COVID-19 vaccine, some staff have left employment in certain facilities due to vaccine mandates. A small, 50-bed nursing home may only have four nurses on staff and if two are unvaccinated and choose to leave their jobs this can have a significant impact on that facility.
Inadequate staffing contributes to increased ED transfers. Staffing levels may also impact the ability of nursing facilities to receive patients from the ED or following a hospital stay.110 While the overall census of most nursing facilities is down, which would indicate a capacity for additional patients, short staffing forces some administrators to pause taking admissions. Patients who are COVID positive can be discharged to nursing facilities, and facilities often create dedicated COVID wings or sections. Depending on whether they have an active outbreak and ability to dedicate staff to the COVID unit, a given facility may decline to accept these transfers. This can lead to longer wait times for patients prior to discharge and have a ripple effect on ED and hospital bed capacity. Further, a patient who meets the criteria for nursing facility level care may refuse to transfer to the setting, which can also delay discharge planning.
Coordinating care at times of transition is a persistent challenge across the healthcare system. Table 4 provides a checklist of factors the ED should consider before transferring back to a long-term care facility. Older adults are particularly vulnerable to adverse events during such care transitions. These may include adverse drug events or medication errors, falls, abuse or neglect, pressure ulcers, and dehydration. The use of systematic approaches, such as checklists and warm handoffs, and calling the next site of care to ensure a coordinated transition, is even more essential.101
Challenging Aspects for Emergency Department Staff
During the COVID-19 pandemic, frequently changing recommendations and requirements from the CDC, CMS, individual state departments of public health, and other agencies have created a particular challenge for the care of patients who are in acute distress, unstable, and require immediate, life-saving treatments.112 Optimizing ED staff and patient safety under those conditions challenges our daily use of personal protective equipment (PPE), types and fit of masks, and frequency of staff testing. Additional issues are caused due to the availability of testing and treatment resources, vaccination and booster requirements, and other public health measures.
ED physicians and nurses, know that the last two years of serving on the frontline of an increasingly strained health care system has been exhausting. Our patients are sick, tired from long waits to be seen, and then are often boarding excessive amounts of time in the ED. It has been challenging if not impossible to care for them in the ways we want and which they deserve.
Our hospitals are strained to the breaking point and often unable to admit those requiring admission nor to support ED staff in managing patients to the extent needed. Many of the community resources we depend on for patient support have closed during COVID-19. We have been asked to keep visitors out of the ED, often causing confrontational conversations with patients’ loved ones. All the while we are worried about getting ill ourselves from a poorly understood or infecting our loved ones with a potentially deadly virus. There are no perfect answers but here are a few best practices shared by our ED colleagues from around the world.
Take care of yourself (self-wellness).
Emergency physicians now rate the highest amongst all specialties in burnout and depression.113 The same may well be true for emergency nurses. We need to recognize just how hard our jobs currently are and take time for wellness activities. Also, we need to encourage our colleagues to do the same.
Bring Caregivers in.
Caregivers (care partners) are not visitors.114 Patients, especially patients with cognitive impairment, need their caregivers. The caregiver is often the ED staff’s best ally and will help in the provision of collateral history as well as in the care of the patient. Caregivers can provide re-orientation, assist with feeding and toileting to decrease delirium development in older patients and stress on ED staff. Help your hospital recognize that caregivers are not visitors by allowing appropriately screened caregivers into the ED with PPE.
Enable everyone on the team to work at the top of their license.
There are many skilled individuals that can help ED performance if we let them. Some EDs are bringing paramedics into the ED to help place IV lines and administer medications.115 Other EDs are using medical or nursing students as vulnerable patient ambassadors who can help ensure that those without caregivers have their needs met. Look around and see who your system can offer to help you. While ED staff often assist with any and all patient care functions as part of the team, it is not optimal to have physicians drawing or sending labs, nor nurses cleaning floors. Keeping professionals functioning at their maximal professional capacity and having adequate support personnel is our goal for both optimal ED functioning and professional satisfaction.
Conclusion
The COVID-19 pandemic has greatly impacted ED care of older adults. Nonspecific symptoms and alterations of mental status are common presentations in both acute and long-haul COVID-19. Categorization into disease severity groups is useful for both treatment and disposition.
Supplemental oxygen is a mainstay of ED stabilization and applies equally to older persons. Vaccinations and boosters are lifesaving and reduce ED visits, especially in those most vulnerable. Strategies to maximize vaccination acceptance and ED distribution of vaccines in older adults should be implemented.
ED providers must have access to multiple external sources to help incorporate the constantly evolving treatments and recommendations, such as monoclonal antibodies and oral antivirals into ED practice. These treatments are particularly useful in the care of older adults with mild to moderate illnesses.
Psychosocial implications, care of those with dementia, and transitions to residential centers are subjects that must be understood by emergency providers in order to provide competent care and dispositions. The optimizing of professional functioning within the ED and maintaining both self-care and care of your colleagues are important for the day-to-day survival of emergency providers under pandemic-induced stress.
Patient Follow Up of Box 1- An Older Patient Presents to the ED for Treatment
- Which medication or treatment could be considered?
This patient had acute onset of symptoms within a few days of presenting to her primary care provider for a routine visit. She had laboratory-confirmed testing for COVID-19. Her vital signs, including pulse oximetry, were normal. There was no sign of delirium, no functional decline, and no worsening of her co-morbid illnesses. The patient had received her vaccination but did not receive her booster. Her age and co-morbidities put her at risk for severe disease. In this case, sotrovimab was available and was administered in the ED. Oral molnupiravir would have been an alternative treatment strategy. - How would you counsel the patient regarding her co-morbid illnesses?
This patient was counseled to continue with her routine medications and monitoring of her blood glucose. Her primary care provider used a secure chat feature in the electronic health record to coordinate a follow-up visit in her office. The patient was encouraged to schedule a COVID-19 booster in the community pharmacy in the next week. Her family was provided the CDC website for guidance regarding their own testing and mask use.
Box 4: Patient Follow Up of Box 2- An Older Patient Presents to the ED for Treatment
- What are common problems for older patients who have recently had COVID-19 infections?
Fatigue, anxiety, dyspnea, and headache are noted as common problems for those who have had COVID-19. These symptoms may be attributed to the long-term scenario of COVID-19. In addition, older adults who have had an acute illness are at risk of functional decline, with or without a COVID-19 illness. Further, a functional decline of an older adult may signal an acute illness or an exacerbation of an underlying condition. A careful history, vital signs, a directed physical examination, and diagnostic evaluation are in order. The ED clinician should concurrently direct attention to her complaint of pain in her legs. - How would you determine the best strategy to help this older patient and her family caregivers?
This individual has several “red flags” which pose risk for her care. She has multiple co-morbid illnesses including dementia and end-stage renal disease. She has not received her COVID-19 vaccination or booster and this poses a particular risk for serious illness. She has missed dialysis in the context of her COVID-19 status. Now she needs more help in transferring from her bed. Her daughter expresses caregiver strain. The best strategy in the ED is to define the underlying problems contributing to her decline. The patient’s preferences for care should be elicited and “What matters most?” Likewise, define if the patient has an advance directive. - How do we access community and long-term services to support this patient and family caregiver?
In this case, the first determination would be if she needs to be admitted or not. The daughter could further describe efforts to access dialysis care. The ED staff should get a sense if the family is able and interested in having the patient return home. With the ED boarding status, a social worker and physical therapist should be consulted while the patient is in the ED.
Keywords
COVID-19, older adult, emergency department care, treatment
Affiliations
Kevin Biese, MD
University of North Carolina Medical School
Alice Bonner, PhD, RN, FAAN
Institute for Healthcare Improvement
Teresita Hogan, MD, FACEP
University of Chicago Medical Center
Michael Malone, MD
Advocate Aurora Health
Patti Pagel, MSN RN GCNS-BC
Advocate Aurora Health
Kathleen Unroe, MD, MHA
Indiana University School of Medicine
IU Center for Aging Research,
Regenstrief Institute
Author Contributions
Corresponding Author: Michael L. Malone, MD: (414) 588-2991, Email: michael.malone.md@aah.org.
Sponsor Role: There were no sponsors of this work.
Funding: There was no funding for this work.
Conflicts of Interest
Michael L. Malone owns stock in Abbott Labs and Abbvie. The authors have declared no conflicts of interest for this article.
Acknowledgments
The authors thank the John A. Hartford Foundation and the West Health Institute for their support for improving emergency care for older Americans.
References
- CORONAVIRUS Resource Center. Johns Hopkins University and Medicine. (online) Available at:
https://coronavirus.jhu.edu/map.html. Accessed March 13, 2022. - Ahmad FB, Cisewski JA, Miniño A, Anderson RN. Provisional Mortality Data – United States, 2020. MMWR Morb
Mortal Wkly Rep. 2021 Apr 9;70(14):519-522. Erratum in: MMWR Morb Mortal Wkly Rep. 2021 Jun 18;70(24):900. . doi:
10.15585/mmwr.mm7014e1. - COVID Data Tracker. Centers for Disease Control and Prevention. https://covid.cdc.gov/covid-data-tracker/#datatrackerhome
- COVID-19 Nursing Home Data updated March 10,2022 (online) Available at https://data.cms.gov/covid-19/covid-19-
nursing-home-data. Accessed March 13,2022. - Grabowski DC, Mor V. Nursing Home Care in Crisis in the Wake of COVID-19. JAMA. 2020 Jul 7;324(1):23-24. doi:
10.1001/jama.2020.8524 - Brown KA, Jones A, Daneman N, et al. Association Between Nursing Home Crowding and COVID-19 Infection and
Mortality in Ontario, Canada. JAMA Intern Med. 2021 Feb 1;181(2):229-236. doi: 10.1001/jamainternmed.2020.6466. - Sarah HY, See I, Kent AG, et al. Characterization of COVID-19 in assisted living facilities—39 states, October
2020. MMWR Morb Mortal Wkly Rep 2020; 69(46): 1730. doi: 10.15585/mmwr.mm6946a3external icon - Fisman DN, Bogoch I, Lapointe-Shaw L, et al. Risk Factors Associated With Mortality Among Residents With
Coronavirus Disease 2019 (COVID-19) in Long-term Care Facilities in Ontario, Canada. JAMA Netw
Open. 2020;3(7):e2015957. doi:10.1001/jamanetworkopen.2020.15957. - Kompaniyets L, Pennington AF, Goodman AB, et al. Underlying Medical Conditions and Severe Illness Among 540,667
Adults Hospitalized With COVID-19, March 2020–March 2021. Prev Chronic Dis 2021;18:210123.
doi: 10.5888/pcd18.210123 - Harrison, S. L., Fazio-Eynullayeva, E., Lane, D. A., et al. Comorbidities associated with mortality in 31,461 adults with
COVID-19 in the United States: A federated electronic medical record analysis. PLoS medicine 2020; 17(9), e1003321.
doi: 10.1371/journal.pmed.1003321external icon
3/24/2022 Review Article 15 | P a g e - Karagiannidis C, Mostert C, Hentschker C, et al. Case characteristics, resource use, and outcomes of 10 021 patients
with COVID-19 admitted to 920 German hospitals: an observational study.Lancet Respir Med. 2020 Sep; 8(9):853-862.
doi: 10.1016/S2213-2600(20)30316-7. - Carpenter CR, Mudd PA, West CP, et al. Diagnosing COVID-19 in the emergency department: A scoping review of
clinical examinations, laboratory tests, imaging accuracy, and biases. Acad Emerg Med. 2020 Aug;27(8):653-670. doi:
10.1111/acem.14048. - Martinez-Fierro ML, Diaz-Lozano M, Alvarez-Zuñiga C, et al. Population-Based COVID-19 Screening in Mexico:
Assessment of Symptoms and Their Weighting in Predicting SARS-CoV-2 Infection. Medicina (Kaunas). 2021;57(4):363.
doi:10.3390/medicina57040363 - Struyf T, Deeks JJ, Dinnes J, et al. Signs and symptoms to determine if a patient presenting in primary care or hospital
outpatient settings has COVID‐19. Cochrane Database of Systematic Reviews 2021, Issue 2. Art. No.: CD013665. doi:
10.1002/14651858.CD013665.pub2. - Factsheet for healthcare providers. COVID-19 RT-PCR Test. Updated April 28, 2021 (online). Available at:
https://www.fda.gov/media/136149/download. Accessed March 13, 2022. - ACEP COVID Management Tool Updated January 13, 2022 (online). Available at: https://www.acep.org/corona/COVID19-alert/covid-19-articles/covid-19-ED-management-tool-now-available/. Accessed March 13, 2022.
- Society of Academic Emergency Medicine COVID-19 Provider Toolkit (online). Available at
https://www.saem.org/education/saem-online-academic-resources/covid-19-provider-toolkit. Accessed March 13, 2022. - Kennedy M, Helfand BKI, Gou RY, et al. Delirium in Older Patients With COVID-19 Presenting to the Emergency
Department. JAMA Netw Open. 2020 Nov 2;3(11):e2029540. doi: 10.1001/jamanetworkopen.2020.29540. - Mahase E. Covid-19: What do we know about “long covid”? BMJ. 2020 Jul 14;370:m2815. doi: 10.1136/bmj.m2815.
- Mirfazeli FS, Sarabi-Jamab A, Pereira-Sanchez V, et al. Chronic fatigue syndrome and cognitive deficit are associated
with acute-phase neuropsychiatric manifestations of COVID-19: A 9-month follow-up study [published online ahead of
print, 2022 Jan 21]. Neurol Sci. 2022;1-9. doi:10.1007/s10072-021-05786-y - Nasserie T, Hittle M, Goodman SN. Assessment of the Frequency and Variety of Persistent Symptoms Among
Patients With COVID-19: A Systematic Review. JAMA Netw Open. 2021;4(5):e2111417.
doi:10.1001/jamanetworkopen.2021.11417 - Cai X, Hu X, Ekumi IO, et al. Psychological Distress and Its Correlates Among COVID-19 Survivors During Early
Convalescence Across Age Groups. Am J Geriatr Psychiatry. 2020 Oct;28(10):1030-1039. doi: 10.1016/j.jagp.2020.07.003. - Justo-Alonso A, García-Dantas A, González-Vázquez AI, et al. How did different generations cope with the COVID-19
pandemic? Early stages of the pandemic in Spain. Psicothema. 2020;32:490–500. doi: 10.7334/psicothema2020.168. - Horn M, Wathelet M, Amad A, et al. Prevalence and Risk Factors of PTSD in Older Survivors of Covid-19 Are The
Elderly so Vulnerable? [published online ahead of print, 2021 Dec 10]. Am J Geriatr Psychiatry. 2021;S1064-
7481(21)00558-3. doi:10.1016/j.jagp.2021.12.005 - Parlapani E, Holeva V, Nikopoulou VA, et al. A review on the COVID-19-related psychological impact on older adults:
vulnerable or not? Aging Clin Exp Res. 2021 Jun;33(6):1729-1743. doi: 10.1007/s40520-021-01873-4. - Nakamura ZM, Nash RP, Laughon SL, Rosenstein DL. Neuropsychiatric Complications of COVID-19. Curr Psychiatry
Rep. 2021 Mar 16;23(5):25. doi: 10.1007/s11920-021-01237-9. - Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder:
retrospective cohort studies of 62,354 COVID-19 cases in the USA. Lancet Psychiatry. 2021;8(2):130–140. doi:
10.1016/S2215-0366(20)30462-4. - Geriatric Emergency care Applied Research GEAR 2.0. Improving care for people with dementia. (Online). Available at
https://gearnetwork.org/about-gear-2/. Accessed March 14, 2022. - Farrell, T.W., Francis, L., Brown, et al. Rationing Limited Healthcare Resources in the COVID-19 Era and Beyond:
Ethical Considerations Regarding Older Adults. J Am Geriatr Soc. 2020; 68: 1143-1149. doi.org/10.1111/jgs.16539 - Hess EP, Grudzen CR, Thomson R, Raja AS, Carpenter CR. Shared Decision-making in the Emergency
Department: Respecting Patient Autonomy When Seconds Count. Acad Emerg Med. 2015 Jul;22(7):856-64. doi:
10.1111/acem.12703 - Hogan TM, Richmond NL, Carpenter CR, et al. Shared Decision Making to Improve the Emergency Care of Older
Adults: A Research Agenda. Acad Emerg Med. 2016 Dec;23(12):1386-1393. doi: 10.1111/acem.13074 - Persad G, Peek ME, Shah SK. Fair Allocation of Scarce Therapies for COVID-19. Clin Infect Dis. 2021 Dec 18:ciab1039.
doi: 10.1093/cid/ciab1039. - Whittle JS, Pavlov I, Sacchetti AD, Atwood C, Rosenberg MS. Respiratory support for adult patients with COVID-19. J
Am Coll Emerg Physicians Open. 2020 Apr 13;1(2):95–101. doi: 10.1002/emp2.12071 - Ulugerger Avci G, Bektan Kanat B, Suzan V, et al. Clinical outcomes of geriatric patients with COVID-19: review of oneyear data. Aging Clin Exp Res. 2022 Jan 22:1–10. doi: 10.1007/s40520-021-02047-y.
- Dondorp AM, Hayat M, Aryal D, et al. Respiratory Support in COVID-19 Patients, with a Focus on Resource-Limited
Settings. Am J Trop Med Hyg. 2020;102(6):1191-1197. doi:10.4269/ajtmh.20-0283
3/24/2022 Review Article 16 | P a g e - Fuentes S., Chowdhury Y. S. (2021). “Fraction of inspired oxygen,” in StatPearls. ed. Emmanuel E. (Treasure Island, FL:
StatPearls Publishing LLC; ). - Lodeserto FJ, Lettich TM, Rezaie SR. High-flow Nasal Cannula: Mechanisms of Action and Adult and Pediatric
Indications. Cureus. 2018 Nov 26;10(11):e3639. doi: 10.7759/cureus.3639. - Chavarria AP, Lezama ES, Navarro MG, et al. High-flow nasal cannula therapy for hypoxemic respiratory failure in
patients with COVID-19. Ther Adv Infect Dis. 2021 Sep 3;8:20499361211042959. doi: 10.1177/20499361211042959. - Alshahrani MS, Alshaqaq HM, Alhumaid J, et al. High-Flow Nasal Cannula Treatment in Patients with COVID-19
Acute Hypoxemic Respiratory Failure: A Prospective Cohort Study. Saudi J Med Med Sci. 2021 Sep-Dec;9(3):215-
222. doi: 10.4103/sjmms.sjmms_316_21 - Lewis SR, Baker PE, Parker R, Smith AF. High-flow nasal cannulae for respiratory support in adult intensive care
patients. Cochrane Database Syst Rev. 2021 Mar 4;3(3):CD010172. doi: 10.1002/14651858.CD010172.pub3. - Singh A, Khanna P, Sarkar S. High-Flow Nasal Cannula, a Boon or a Bane for COVID-19 Patients? An Evidence-Based
Review. Curr Anesthesiol Rep. 2021 Mar 2:1-6. doi: 10.1007/s40140-021-00439-4. - Ospina-Tascón GA, Calderón-Tapia LE, García AF, et al and the HiFLo-Covid Investigators. Effect of High-Flow Oxygen
Therapy vs Conventional Oxygen Therapy on Invasive Mechanical Ventilation and Clinical Recovery in Patients With
Severe COVID-19: A Randomized Clinical Trial. JAMA. 2021 Dec 7;326(21):2161-2171. doi: 10.1001/jama.2021.20714. - Veronese N, Petrovic M, Benetos A, at al; special interest group in Systematic Reviews and Meta-analyses and the task
force on Pharmaceutical strategy of the European Geriatric Medicine Society (EuGMS). Underrepresentation of older
adults in clinical trials on COVID-19 vaccines: A systematic review. Aging Res Rev. 2021 Nov;71:101455. doi:
10.1016/j.arr.2021.101455. - Antonelli Incalzi R., Trevisan C., Del Signore S., et al. Are vaccines against COVID-19 tailored to the most vulnerable
people? Vaccine. 2021;39(17):2325–2327. doi: 10.1016/j.vaccine.2021.03.066. - Salmerón Ríos S., Mas Romero M., Cortés Zamora E.B., et al. Immunogenicity of the BNT162b2 vaccine in frail or
disabled nursing home residents: COVID-A study. J Am Geriatr Soc 2021;69(6):1441–1447. doi: 10.1111/jgs.17153. - COVID-19 Vaccination demographics in the United States- Updated Mach 13, 2022 (Online). Available at:
https://data.cdc.gov/Vaccinations/COVID-19-Vaccination-Demographics-in-the-United-St/km4m-vcsb/data. Accessed
March 14, 2022. - Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2
infections and COVID-19 cases, hospitalizations, and deaths following a nationwide vaccination campaign in Israel: an
observational study using national surveillance data. Lancet. 2021 May 15; 397(10287):1819-1829. Erratum in: Lancet.
2021 Jul 17;398(10296):212. doi: 10.1016/S0140-6736(21)00947-8. - Thompson MG, Stenehjem E, Grannis S, Ball SW, et al. Effectiveness of Covid-19 Vaccines in Ambulatory and Inpatient
Care Settings. N Engl J Med 2021; 385:1355-1371 doi: 10.1056/NEJMoa2110362. - Wang SY, Juthani PV, Borges KA, et al. Severe breakthrough COVID-19 cases in the SARS-CoV-2 delta (B.1.617.2)
variant era. Lancet Microbe. 2022 Jan;3(1):e4-e5. doi: 10.1016/S2666-5247(21)00306-2. - Teran R.A., Walblay K.A., Shane E.L. et al. Post vaccination SARS-CoV-2 Infections Among Skilled Nursing Facility
Residents and Staff Members – Chicago, Illinois, December 2020-March 2021. MMWR. Morbidity and mortality weekly
report. 2021;70(17):632–638. - Bar-On YM, Goldberg Y, Mandel M, et al. Protection against Covid-19 by BNT162b2 Booster across Age Groups. N Engl
J Med. 2021 Dec 23;385(26):2421-2430. doi: 10.1056/NEJMoa2115926. - Minjie Li, Juan Yang, Lin Wang, et al. A booster dose is immunogenic and will be needed for older adults who have
completed two doses vaccination with CoronaVac: a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial.
medRxiv 2021.08.03.21261544; doi:10.1101/2021.08.03.21261544v1 - Andrews N, Tessier E, Stowe J, Grower C et al. Duration of Protection against Mild and Severe Disease by Covid -19
Vaccine. N Engl J Med 2022; 386:340-350. doi: 10.1056/NEJMoa2115481. - Tenforde MW, Self WH, Adams K, et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and
Disease Severity. JAMA. 2021;326(20):2043–2054. doi:10.1001/jama.2021.19499. - Tenforde MW, Patel MM, Gaglani M, et al. Effectiveness of a Third Dose of Pfizer-BioNTech and Moderna Vaccines in
Preventing COVID-19 Hospitalization Among Immunocompetent and Immunocompromised Adults – United States,
August-December 2021. MMWR Morb Mortal Wkly Rep. 2022 Jan 28;71(4):118-124. doi: 10.15585/mmwr.mm7104a2.
PMID: 35085218. - Danza P, Koo TH, Haddix M, et al. SARS-CoV-2 Infection and Hospitalization Among Adults Aged ≥18 Years, by
Vaccination Status, Before and During SARS-CoV-2 B.1.1.529 (Omicron) Variant Predominance – Los Angeles County,
California, November 7, 2021-January 8, 2022. MMWR Morb Mortal Wkly Rep. 2022 Feb 4;71(5):177-181. doi:
10.15585/mmwr.mm7105e1. - Arbel R, Hammerman A, Sergienko R, et al. BNT162b2 Vaccine Booster and Mortality Due to Covid-19. N Engl J Med.
2021 Dec 23;385(26):2413-2420. doi: 10.1056/NEJMoa2115624.
3/24/2022 Review Article 17 | P a g e - Amirthalingam G, Bernal JL, Andrews NJ, et al. Serological responses and vaccine effectiveness for extended COVID-19
vaccine schedules in England. Nat Commun 2021;12:7217-7217. doi: 10.1038/s41467-021-27410-5. Erratum in: Nat
Commun. 2022 Feb 2;13(1):733. - Costa Clemens SA, Weckx L, Clemens R, et al. Heterologous versus homologous COVID-19 booster vaccination in
previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): a phase 4, non-inferiority, singleblind, randomised study. Lancet. 2022 Jan 21;399(10324):521–9. doi: 10.1016/S0140-6736(22)00094-0. - Pfizer and BioNTech seek authorization of a second booster shot for older Americans March 15, 2022 (Online) Available
at: https://www.nytimes.com/2022/03/15/us/politics/pfizer-second-booster-shot-older-americans.html. Accessed March 16,
2022. - Glenton C, Carlsen B, Lewin S, et al and the VITAL consortium. Healthcare workers’ perceptions and experiences of
communicating with people over 50 years of age about vaccination: a qualitative evidence synthesis. Cochrane Database
Syst Rev. 2021 Jul 20;7(7):CD013706. doi: 10.1002/14651858.CD013706.pub2. - Connors J, Bell MR, Marcy J, et al. The impact of immuno-aging on SARS-CoV-2 vaccine development. Geroscience.
2021;43(1):31-51. doi:10.1007/s11357-021-00323-3. - Privor-Dumm LA, Poland GA, Barratt J, et al. A global agenda for older adult immunization in the COVID-19 era: A
roadmap for action. Vaccine. 2021;39(37):5240-5250. doi:10.1016/j.vaccine.2020.06.082 - ACEP COVID-19 Field Guide (online). Available at: https://www.acep.org/corona/covid-19-field-guide/specialpopulations/elderly-patients. Accessed March 10, 2022.
- *IDSA Guidelines on the Treatment and Management of Patients with COVID-19. The Infectious Disease Society of
America. Updated 2-16-2022 (online). Available at https://www.idsociety.org/COVID19guidelines. Accessed March 10,
2022. - **Coronanavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health (online). Available at:
https://www.covid19treatmentguidelines.nih.gov/. Accessed March 10, 2022. - ESCMID Covid-19 Living Guidelines (online). Available at:
https://reader.elsevier.com/reader/sd/pii/S1198743X21006340?token=6BD5B5441DDA4741000D2F4B742D02B5BA1E07
85C77228F949A59439262B5F3D13823A5960D96D17FA9A71731A30C4E3&originRegion=us-east1&originCreation=20220128153841. Accessed March 10, 2022. - World Health Organization Living COVID-19 Guidelines (online). Available at:
https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2022.1. Accessed March 10, 2022. - Federal Response to COVID-19: Therapeutics Clinical Implementation Guide, 1-10-2022 Outpatient administrative
guide for healthcare providers (online). Available at: https://aspr.hhs.gov/COVID-19/Therapeutics/Documents/USGCOVID19-Tx-Playbook.pdf. Accessed March 10, 2022. - Side-by-Side Overview of Outpatient Therapies Authorized for Treatment of Mild- Moderate COVID-19 (online).
Available at https://aspr.hhs.gov/COVID-19/Therapeutics/Documents/side-by-side-overview.pdf. Accessed March 10,
2022. - Chen P, Nirula A, Heller B,et al. SARS-CoV-2 neutralizing antibody LY-CoV555 in outpatients with COVID-19. N Engl J
Med 2021; 384:229-237. doi: 10.1056/NEJMoa2029849. - Weinreich DM, Sivapalasingam S, Norton T, et al. REGN-COV1, a neutralizing antibody cocktail, in outpatients with
COVID-19. N Engl J Med 2021;384:238-251. doi: 10.1056/NEJMoa2035002. - Gottlieb RL, Nirula A, Chen P, et al. Effect of bamlaniviman as monotherapy or in combination with Etesevimab on viral
load in patients with mild to moderate COVID-19: a randomized clinical trial. JAMA 2021;325(7): 632-644. doi:
10.1001/jama.2021.0202. - Bariola JR, McCreary EK, Wadas RJ, et al. Impact of monoclonal antibody treatment on hospitalization and mortality
among non-hospitalized adults with SARS-CoV-2 infection. medRxiv 2021, 10.1101/2021.03.25.21254322. - Gupta A, Gonzalez-Rojas Y, Juarez E, et al and the COMET-ICE Investigators. Early Treatment for Covid-19 with
SARS-CoV-2 Neutralizing Antibody Sotrovimab. N Engl J Med. 2021 Nov 18;385(21):1941-1950. doi:
10.1056/NEJMoa2107934. - State/ Territory Coordinated Distribution of COVID-19 Therapeutics. Available at:
https://www.phe.gov/emergency/events/COVID19/therapeutics/distribution/Pages/data-tables.aspx. Accessed February
10, 2022. - Burki TK. The role of antiviral treatment in the COVID-19 pandemic [published online ahead of print, 2022 Jan
13]. Lancet Respir Med. 2022;S2213-2600(22)00011-X. doi:10.1016/S2213-2600(22)00011-X - Jayk Bernal A, Gomes da Silva MM, Musungaie DB, et al. and the MOVe-OUT Study Group. Molnupiravir for Oral
Treatment of Covid-19 in Non-Hospitalized Patients. N Engl J Med. 2022 Feb 10;386(6):509-520. doi:
10.1056/NEJMoa2116044. - Singh AK, Singh A, Singh R, Misra A. An updated practical guideline on use of molnupiravir and comparison with
agents having emergency use authorization for treatment of COVID-19. Diabetes Metab Syndr. 2022 Jan
13;16(2):102396. doi: 10.1016/j.dsx.2022.102396.
3/24/2022 Review Article 18 | P a g e - Dyer O. Covid-19: FDA expert panel recommends authorizing molnupiravir but also voices concerns. BMJ. 2021 Dec
2;375:n2984. doi: 10.1136/bmj.n2984. - Gottlieb RL, Vaca CE, Paredes R, et al and the PINETREE Investigators.
Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. N Engl J Med. 2022 Jan 27;386(4):305-315.
doi: 10.1056/NEJMoa2116846. - Beigel JH, Tomashek KM, Dodd LE, et al. and the ACTT-1 Study Group Members. Remdesivir for
the Treatment of Covid-19 – Final Report. N Engl J Med. 2020 Nov 5;383(19):1813-1826. doi: 10.1056/NEJMoa2007764. - Ansems K, Grundeis F, Dahms K, et al. Remdesivir for the treatment of COVID-19. Cochrane Database Syst Rev. 2021
Aug 5;8(8):CD014962. doi: 10.1002/14651858.CD014962. - Ohl ME, Miller DR, Lund BC, et al. Association of Remdesivir Treatment With Survival and Length of Hospital Stay
Among US Veterans Hospitalized With COVID-19. JAMA Netw Open. 2021 Jul 1;4(7):e2114741. doi:
10.1001/jamanetworkopen.2021.14741. - Libster R, Perez Marc G, Wappner D, et al. Early high-titer plasma therapy to prevent severe Covid-19 in older adults.
N Engl J Med 2021;384: 610-618. doi: 10.1056/NEJMoa2033700 - Chai KL, Valk SJ, Piechotta V, et al. Convalescent plasma or hyper immune immunoglobulin for people with COVID-19:
a living systematic review. Cochrane Database Syst Rev. 2020 Oct 12;10:CD013600. doi:
10.1002/14651858.CD013600.pub3. Updated in: Cochrane Database Syst Rev. 2021 May 20;5:CD013600. PMID:
33044747. - Esmaeili B, Esmaeili S, Pourpak Z. Immunological effects of convalescent plasma therapy for coronavirus: a scoping
review. BMC Infect Dis. 2021 Dec 24;21(1):1278. doi: 10.1186/s12879-021-06981-0. - RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid-19. N
Engl J Med. 2021 Feb 25;384(8):693-704. doi: 10.1056/NEJMoa2021436. - Albarrán-Sánchez A, Ramírez-Rentería C, Mercado M, et al. Real-world evidence of the use of glucocorticoids for severe
COVID-19. Ther Adv Endocrinol Metab. 2022 Jan 19;13:20420188211072704. doi: 10.1177/20420188211072704. - Wu B. Social isolation and loneliness among older adults in the context of COVID-19: a global challenge. Glob Health Res
Policy. 2020 Jun 5;5:27. doi: 10.1186/s41256-020-00154-3. - COVID driven isolation can be dangerous for older adults from the National Council of Aging (online). Available at
https://www.ncoa.org/article/covid-driven-isolation-can-be-dangerous-for-older-adults. Accessed February 12, 2022. - O’Brien K, Light SW, Bradley S, Lindquist L. Optimizing voice-controlled intelligent personal assistants for use by
home-bound older adults. J Am Geriatr Soc. 2022 Jan 14. doi: 10.1111/jgs.17625. - Elman A, Baek D, Gottesman E, et al. Unmet needs and social challenges for older adults during and after the COVID19 Pandemic: An opportunity to improve care. Journal of Geriatric Emergency Medicine. 2021: Vol 2(11) article 1.
- Fulmer T, Mate KS, Berman A. The Age-Friendly Health System Imperative. J Am Geriatr Soc. 2018 Jan;66(1):22-
24. doi: 10.1111/jgs.15076 - 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. 2021 Mar;17(3):327-406. doi: 10.1002/alz.12328.
- Daras LC, Feng Z, Wiener JM, Kaganova Y. Medicare Expenditures Associated With Hospital and Emergency
Department Use Among Beneficiaries With Dementia. Inquiry. 2017 Jan;54:1-9. doi: 10.1177/0046958017696757. - Sleeman KE, Perera G, Stewart R, Higginson IJ. Predictors of emergency department attendance by people with
dementia in their last year of life: Retrospective cohort study using linked clinical and administrative data. Alzheimers
Dement. 2018 Jan;14(1):20-27. doi: 10.1016/j.jalz.2017.06.2267. - MacNeil-Vroomen JL, Nagurney JM, Allore HG. Comorbid conditions and emergency department treat and release
utilization in multimorbid persons with cognitive impairment. Am J Emerg Med. 2020 Jan;38(1):127-131. doi:
10.1016/j.ajem.2019.07.023. - Kim J, Lee S, Pfau N, et al. The Double Burden of Depression and Social Isolation in Older Adults during the COVID-19
Pandemic. Poster Number NR-6. American Journal of Geriatric Psychiatry. April 2021; 29: 4S, S108-S109. - Kotwal AA, Holt-Lunstad J, Newmark RL, et al. (2021). Social Isolation and Loneliness among San Francisco Bay Area
Older Adults during the COVID-19 Shelter-in-Place Orders. J Am Geriatr Soc. 2021 Jan;69(1):20-29. doi: 10.1111/jgs. - Batsis JA, Daniel K, Eckstrom E, et al. Promoting Healthy Aging during COVID-19. J Am Geriatr Soc. 2021
Mar;69(3):572-580. doi: 10.1111/jgs.17035. - Bass DM, Judge KS, Maslow K, et al. Impact of the care coordination program “Partners in Dementia Care” on veterans’
hospital admissions and emergency department visits. Alzheimers Dement (N Y). 2015 Apr 17;1(1):13-22. doi:
10.1016/j.trci.2015.03.003. - Franzosa E, Gorbenko K, Brody AA, et al. “At Home, with Care”: Lessons from New York City Home-based Primary
Care Practices Managing COVID-19. J Am Geriatr Soc. 2021 Feb;69(2):300-306. doi: 10.1111/jgs.16952. - Morris AM, Engelberg Anderson JK, Schmitthenner B, et al. Leveraging emergency department visits to connect older
adults at risk for malnutrition and food insecurity to community resources: design and protocol development for the
BRIDGE study. Pilot Feasibility Stud 2020; 6: 36. https://doi.org/10.1186/s40814-020-00576-3.
3/24/2022 Review Article 19 | P a g e - Gautun H, Bratt C. Caring too much? Lack of public services to older people reduces attendance at work among their
children. Eur J Ageing. 2017; 14: 155-166. doi: 10.1007/s10433-016-0403-2. - DeDonato E, Hall SE, Hogan TM, Gleason LJ. Interprofessional Education of Emergency Department Team on Falls in
Older Adults. J Am Geriatr Soc. 2020 Mar;68(3):E7-E9. doi: 10.1111/jgs.16358.
1 - Loomer L, Grabowski DC, Yu H, Gandhi A. Association between nursing home staff turnover and infection control
citations. Health Serv Res. 2021 Sep 6. doi: 10.1111/1475-6773.13877. - Gandhi A, Yu H, Grabowski DC. High Nursing Staff Turnover In Nursing Homes Offers Important Quality Information.
Health Aff (Millwood). 2021 Mar;40(3):384-391. doi: 10.1377/hlthaff.2020.00957. - Bernstein L, Van Dam A. Nursing home staff shortages are worsening problems at over- whelmed hospitals. The
Washington Post, December 28, 2021 and updated January 7,2022 (online). Available at
https://www.washingtonpost.com/health/2021/12/28/nursing-home-hospital-staff-shortages/. Accessed 2-16-2022. - Burkett E, Carpenter CR, Hullick C, Arendts G, Ouslander JG. It’s time: Delivering optimal emergency care of
residents of aged care facilities in the era of COVID-19. Emerg Med Australas. 2021 Feb;33(1):131-137. doi:
10.1111/1742-6723.13683. - Levine S, Bonner A, Perry A, et al. COVID-19 in older adults: Transfers between nursing homes and hospitals. JGEM
2020;1(5):1-7. (online) Available at https://gedcollaborative.com/jgem/vol1-is5-covid-19-older-adults-transfers-betweennursing-homes-and-hospitals/. Accessed February 16,2022. - Wells, CM, Zhang, Z, Spano-Szekely, L, Siller, J, Brannon, H, Schulz, K, Scott, C, Dolphy, M, Hughes, E, Kohli-Seth, R.
(2021). Tiered Model of Nursing Staffing for Critical Care and the Emergency Departments in the Wake of a Pandemic.
JONA. 51:2; E1-E5. doi: 10.1097/NNA.0000000000000979. - Emergency physicians’ level of burnout jumped last year. Health Care Dive January 24,2022. (online). Available at:
https://www.healthcaredive.com/news/burnout-emergency-physicians-rising/617554/. Accessed February 15,2022. - Reinhard S, Drenkard K, Choula R, Curtis A. They’re Not Visitors: COVID-19 Visitor Restrictions Highlight Need For
Change. AARP Blog, July 28, 2020 (online) Available at: https://blog.aarp.org/thinking-policy/theyre-not-visitors-covid-19-
visitor-restrictions-highlight-need-for-change. Accessed February 15,2022. - Hollander JC, Sharma R. The Availablists: Emergency care without the emergency department NEJM Catalyst 2021.
DOI: 1056.21.0310. (online) Available at: https://catalyst.nejm.org/doi/pdf/10.1056/CAT.21.0310. Accessed March 14,
2022.