Abstract
Background
COVID-19 has led to a dramatic increase in the use of telehealth services, particularly with older adults, who are at highest risk of potential infection and mortality. As a result, Emergency Departments (EDs) around the country are now leveraging telehealth as a key tool in a variety of settings for COVID-19 and non-COVID related conditions.
Participants
Three EDs participating in the San Diego, California Senior Emergency Care Initiative, and the EDs of Dartmouth-Hitchcock in Lebanon, New Hampshire, Sinai Health in Toronto, Canada, and Washington University in St. Louis, Missouri contributed to this report. We outline 3 specific models illustrating how telehealth is being used to increase access and care for older adults during COVID-19. In each model we emphasize needs of unique populations, and provide example workflows, and staffing considerations.
Real-world examples
First, in nursing homes a primary goal is to determine if facilities can treat in place, or transfer. A common approach is a provider-to-provider model where EDs consult directly with nursing home providers. Second, in rural and critical access hospitals telehealth can provide access to multi-specialty expertise when managing complex patients. In rural settings, establishing a new telehealth program may not be feasible. However, partnering with an organization that already has an existing telehealth platform is the fastest route to implementation. Finally, telehealth can be used for forward triage in primary and ED settings. The forward triage focus is on prioritizing which patients can be seen virtually and, if needed, determining the ED or other site as the best location for care.
Conclusions
As telehealth utilization increases during COVID-19, telehealth can maintain medical contact while helping decrease spread of infection during this public health crisis. Addressing the healthcare needs of vulnerable seniors by virtual connection minimizes exposure to infection for patients and ED providers, positioning telehealth as a critical tool in combating the current pandemic.
Key Words
Geriatrics, COVID-19, Telehealth, Post-acute, Rural, Forward triage
Box 1
Clinical Case
A 25-bed community-based Emergency Department (ED) is located 100 miles from the nearest academic medical center. The community-based ED is the only ED within a 50-mile radius and serves a local rural population as well as 15 nursing homes in the area. The ED Medical Director is concerned that her already understaffed ED will be overwhelmed in the coming weeks with an anticipated surge in visits from COVID-19. She is aware that telehealth may be an important tool in triaging and treating patients, and in general is currently reimbursable.
- What telehealth protocols and programs should be implemented to help reduce overcrowding?
- How can the Medical Director incorporate forward triage across a variety of settings?
- How can ED’s address the needs of the community while protecting their own staff?
- Given limited resources and time, what options does the Medical Director have?
- What guidance can the Medical Director establish to help her clinicians provide care via telehealth?
What is Telehealth & Forward Triage?
The Office of the National Coordinator for Health Information Technology (ONC), broadly defines telehealth as the use of electronic information and technologies to support and promote long-distance clinical care, patient and professional health-related education, public health and health administration.1 Forward triage is the sorting of patients based on needs before potential ED transfer. Forward triage establishes who requires ED treatment, prioritizes care delivery, and determines appropriateness of treatment in place, or in other settings.2 This paper highlights different models of how telehealth is being deployed by ED’s around the country based on needs, clinical setting, and resources.
Why Telehealth & Older Adults?
The COVID-19 pandemic has led to a dramatic increase in the use of telehealth services. Telehealth may be particularly useful to limit spread and treat infection in older adults, who are at highest risk of mortality from COVID-19. With the delay or cancellation of non-essential clinical services, and decreased ED use due to infection concerns, telehealth has emerged as a critical tool. Telehealth can reduce ED overcrowding, increase virtual ED access, and incorporate forward triage to prioritize which patient needs to be seen in the ED, and who can be treated in place or other settings.2
Reimbursement & Regulatory Challenges
Historically, the Social Security Act has governed what telehealth services are and are not covered under Medicare. The statutory conditions have long been identified as significant limitations to the creation and adoption of telehealth services. The more notable restrictive stipulations are that beneficiaries need to be located in a qualifying rural area, within a specific qualifying originating site, and services delivered by an approved distant site provider. Compounded by regulatory barriers around compliance with the Health Insurance Portability and Accountability Act of 1996 (HIPAA), interstate licensure requirements, and change management at the practice level, these barriers have all limited the use of telehealth. Given the current pandemic, the federal government has temporarily lifted or waived many of these barriers. Key changes include:
- all eligible Medicare beneficiaries can receive telehealth, and providers can be reimbursed at the same rate as an in-person visit and is retroactive to March 1, 2020.
- the Office of Civil Rights (OCR), responsible for enforcing certain regulations under HIPAA, will exercise enforcement discretion and not impose penalties for noncompliance under the good faith provision during the public health emergency.
- providers can leverage a variety of different technologies such as FaceTime and Skype to facilitate visits.
- many states are also lifting or relaxing long standing policy and regulations to provide care during this state of emergency.
- common ED billing codes for the evaluation and management of services in the ED (CPT codes: 99281 – 99285) are now billable as telehealth as long as visits are marked with billing code modifier 95, which indicates services were rendered via telehealth.
Equally important, many private health insurers have implemented changes to accommodate telehealth visits. Specific details on access to telehealth, coding and billing for telehealth, as well as coverage for providers and members. This can be found at the American College of Emergency Physicians (ACEP) COVID-19 Insurance Policy webpage.3
Real World Examples
While reimbursement and regulatory restrictions have been temporarily lifted, launching a telehealth program during COVID-19 can seem daunting. Below are 3 examples and key considerations on how telehealth is being utilized during the pandemic.
1. Telehealth with Nursing Homes
The need: While the majority of attention has focused on hospitals and ED’s during COVID-19, the need for telehealth may be greatest in nursing homes. Nursing homes often lack financial resources, have few covering providers, high staff turnover, and may lack adequate infection control measures and equipment. Generally speaking, nursing homes are considered high-risk settings for severe outbreaks given the advanced age, and multiple comorbidities of residents.4 Given limited capacity and capability to address the needs of this high-risk population, before and after an acute care response, managing COVID-19 in nursing homes is particularly challenging.5
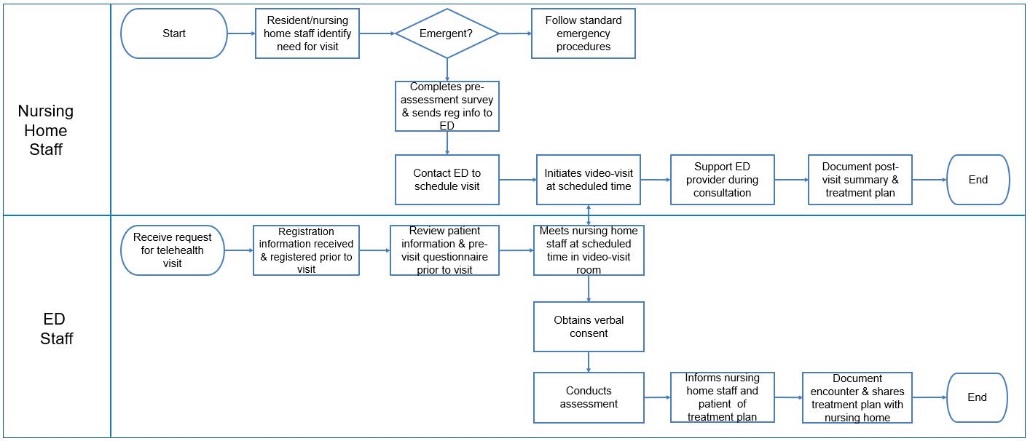
Example- San Diego County Senior Emergency Care Initiative: One example of how telehealth is being used to connect nursing homes and EDs is the San Diego County Senior Emergency Care Initiative. This initiative is a public/private partnership where all major Health Systems across the County pledged to become senior-friendly EDs. In San Diego County, 3 EDs (and counting) have connected with over 12 local nursing homes via telehealth to help assess whether the residents can be treated in place or need to be transferred.6 The workflow below outlines an example of how nursing homes are working with EDs throughout the county. *See Appendix 1
Staffing Considerations: The ability to facilitate telehealth visits with ED providers varies based on the level of clinical personnel available at the nursing home as well as the needs of the facility. However, in all cases, the nursing home needs to establish a tele-presenter. For example, a Certified Nurse Assistant, Registered Nurse, Emergency Medical Technician, or similar person. This individual must have received appropriate training to facilitate telehealth visits while standing alongside the resident/patient. In the model being deployed across San Diego County can take up to 2 weeks to implement depending on the type of services and how often they are needed. For instance, nursing homes requesting 24/7 availability to an ED provider will have to consider who at the nursing home will facilitate visits during off hours and whether any modifications to workflows are necessary.
For EDs, telehealth can be facilitated by a variety of providers depending on the needs of the nursing home. For example, registered nurses, advanced practice providers (APP), or ED physicians are all commonly used to provide telehealth visits for nursing home residents. For urgent/non-emergent telehealth consultations EDs may opt for an initial nurse triage to determine if additional clinical consultation is necessary with an on-call ED physician as needed. In each implementation, the nursing home initiates contact with the ED, unless it is considered an emergent condition at which point the nursing home follows existing protocols.
One of the most impactful models is a provider-to-provider approach where the ED provides supportive consultation directly to the Medical Director and/or clinical leadership of a nursing home. Nursing home Medical directors are often responsible for several sites and hundreds of patients, making care during a pandemic especially challenging. By providing an ED consultation via telehealth, the ED and nursing home providers are able to ensure residents have timely access to a provider should the Medical Director or resident’s primary care physician not be available. Furthermore, provider-to-provider consultations are now also eligible for reimbursement, regardless of modality by telephone, video platform, or another modality.
When facilitating telehealth visits between the ED and nursing home, communication between leadership at each site (e.g. ED Medical Director, nursing home Medical or Nursing Director) is important to collectively determine which patients can be treated onsite, and which require transfer to the ED. This is especially important when COIVD-19 is a diagnostic consideration, to ensure appropriate infection prevention measures are in place.
2. Rural and Critical Access Hospitals
The need: Prior to the current pandemic, the increasing shortage of healthcare professionals in the United States presented a challenge for many organizations, with rural facilities most harshly impacted. Approximately 20 percent of Americans live in rural areas, though only 10% of physicians practice in those regions.7 For example, in the northern New England states of Maine, New Hampshire, and Vermont, 1.9 million people live in rural areas and 50% of hospitals are Critical Access. This is in contrast to 25% nationally. These challenges disproportionately affect rural populations since they tend to be older, have more medical comorbidities, lower mean socioeconomic status, and longer travel times to specialty care.8,9 Many of the challenges of rural health care for older Americans, including those of access to care, can be mitigated through telehealth.
Example- Dartmouth-Hitchcock TeleEmergency Service: As a leader in New England, the Dartmouth-Hitchcock (D-H) Center for Telehealth was founded in 2012 to provide telehealth services to the surrounding region, including emergency care via its TeleEmergency service. The D-H TeleEmergency service brings an on-demand D-H ED physician and nurse to join the facilities patient-bedside team of a rural hospital ED site, virtually via high-quality two-way interactive audio-video communication from a dedicated Hub.
Hospitals participating in the service, all of which are located rurally, designate two high acuity ED rooms to be hard-wired with a call button on the wall, monitor, high-definition camera, video codec device to help decompress large files, speaker, and a microphone. At any given time, any member of the rural ED team can have immediate access to the D-H TeleEmergency team. For this type of pre COVID-19 service, implementation, which we describe below, would normally take at least 75 days, however, an accelerated process is described below.
Given the current pandemic, independently establishing a new TeleEmergency “Hub” is likely impractical. However, partnering with an organization that has an established telehealth program can accelerate this process to a matter of weeks. To accelerate the process, the D-H team eliminated the majority of implementation meetings, streamlined contracting, took advantage of the removal of typical credentialing barriers, minimized electronic health record (EHR) integration, and performed ongoing training and relationship building over the camera after “go-live”. Partnering with an already established telehealth organization may be particularly helpful not only to ensure that enhanced geriatric care is delivered, but also to help decide when to transfer patients to higher levels of care while ensuring a thorough goals of care conversation occurs. The model below follows 4 broad steps:
Table 1
The Standard Clinical Workflow
- Call initiation
- A member of the local bedside team initiates a request with the Hub site via phone call which goes directly to the hub.
- The bedside team can immediately return to care of the patient.
- The Hub team answers the call and conducts a brief assessment to understand:
- hospital name
- specific ED room/location
- chief complaint or the equivalent (optional)
- initial level of support requested, for example, nursing only, nurse and physician, physician only, transfer assistance, or other. Keep in mind the support type can change during the encounter.
- The Hub team contacts the site within 60 seconds of receiving a call and initiates live interactive audiovisual communication via tablet using an existing video platform.
- Ongoing collaborative support
- The Hub team:
- performs ongoing collaborative assistance to the bedside team and/or directs care as per the request and the patient’s condition.
- performs ongoing documentation of the encounter.
- The Spoke team:
- typically includes a nurse and an ED provider (physician or associate provider) who performs the majority of bedside care, including placing IV’s, and administering medications.
- relays to the Hub team via live audiovisual communication details that are not easily viewable by the Hub team; (the Hub team view vital signs and cardiac monitor and can often determine overall degree of illness/injury, respiratory distress, description of wounds, and so on.)
- The Hub team:
- Transfer and transport
- If patient transfer to another facility is needed at any point, the Hub team:
- identifies/finds an appropriate facility that has capability and capacity.
- gains acceptance at the receiving facility on behalf of the bedside team.
- performs doc-to-doc and nurse-to-nurse report.
- coordinates transport if requested.
- If patient transfer to another facility is needed at any point, the Hub team:
- Post-encounter
- Documentation is sent to the site within 10 minutes for review and for EHR upload.
Staffing Models: The model above is an example of a “hub and spoke” approach in providing services to surrounding rural or critical access hospitals or spoke sites. The D-H TeleEmergency service utilizes both an Emergency Medicine (EM) trained physician and nurse to join the bedside team virtually and is staffed 24/7 to offer assistance for the following:
- nursing documentation and support
- assistance with codes, traumas, and critically ill patients
- medication questions
- procedural guidance
- managing patient care primarily
- providing a second opinion
- coordinating transfers and transport to the D-H hub
3. Forward Triage
The need: The current pandemic has delayed and/or cancelled many standard care and elective procedures. Older people who are already at heightened risk for infection are particularly impacted. To help keep patients connected with providers, health systems have turned to use of forward triage for both acute and non-acute conditions. Forward triage has many advantages beyond essential physical distancing. For example, multiple handoffs can be avoided as well as transportation and cross-contamination risk between patients and staff. Additionally, physically moving older adults can be expensive, challenging, and potentially harmful by increasing risk of falls and incident delirium.10,11 Finally, forward triage helps to limit hospital surges exposing patients to COVID-19 during long waiting room times and conserves personal protective equipment (PPE) for staff. Below are 2 examples of forward triage; within primary care and an ED setting.
Primary Care: Family Medicine at Sinai Health in Toronto, Canada operates 2 family health team locations, one a community practice and the other an academic practice that offers primary care services to people of all ages through interdisciplinary teams. Approximately 19,000 patients are registered to the 2 sites. The COVID-19 pandemic quickly changed the service delivery model for patients with approximately 90% of visits becoming virtual visits. Only 10% required an in-person visit, allowing presence of a much smaller “skeleton staff” in the office. The forward triage strategy was launched with five goals:
- Identifying patients who will always require in-person visits without being converted to telehealth visits. For example, prenatal, newborns, and visits requiring immunizations.
- Conducting phone screening of all in-person visits for COVID-19 symptoms the day before or day of an in-person visit.
- Giving clear instructions to reception staff to book all visits as telehealth visits, while excluding a defined list of required in-person visits.
- Transferring all patients with respiratory symptoms or more urgent matters to a nurse for telephone triage and possible referral to the ED.
- Establishing a new scheduling template in the electronic health record (EHR) to indicate virtual or in-person visits.
To launch a forward triage program, at minimum telephone access and/or video visit technology are required. For phone visits, first determine the most efficient way to forward office calls to a remote setting. To avoid forwarding calls to a personal mobile device, a separate mobile device can be purchased with an unlimited voice plan. If using a personal device, be sure caller ID is blocked when facilitating telehealth visits.
For video visits a computer with webcam and audio is required either through the computer or via external speakers. A hard-wired network is recommended for privacy. Desktop computers with a large screen are recommended vs. laptop computers which have smaller screens and lower resolution. If a secure electronic health record cannot be accessed remotely, use a secure USB key that encrypts data.
Staffing Model: An interdisciplinary team is utilized across the forward triage strategy to provide virtual clinical care in most cases, and in-person when required. Central to the forward triage strategy is the nursing staff to manage initial triage calls. When call volume reaches capacity, medical residents or physicians who are on quarantine, as well as staff with pre-existing conditions or higher risk for patient-facing care, are re-deployed to telephone triage to increase capacity.
In addition to clinical staff, telehealth should also be leveraged for interprofessional health providers such as physical therapy, pharmacy, case management, and others allowing for continuity of services.
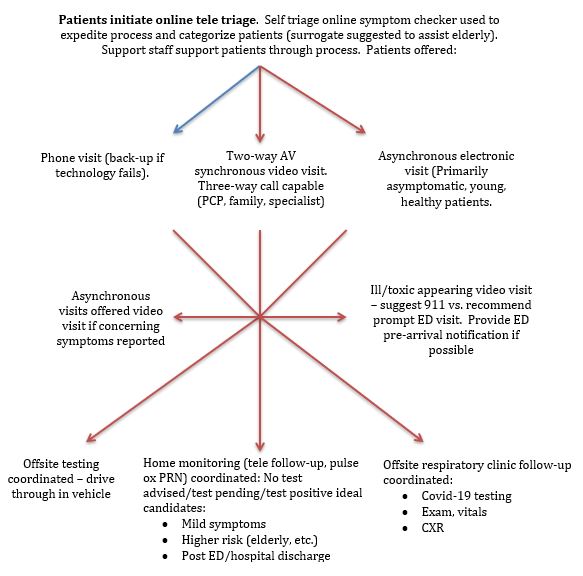
Emergency Department: Barnes Jewish Christian (BJC) health system in Saint Louis, Missouri, in collaboration with Washington University in St. Louis was able to develop a rapid model, over a course of a few weeks. This virtual care operation incorporated forward triage to prepare for and help mitigate, any COVID-19 surge. The program was integrated into the existing EHR and the existing telehealth platform to jumpstart the virtual care service. In the BJC model, patients access an online portal to initiate self-triage where a symptom checker helps sort patients for appropriate telehealth visit type. Then, asynchronous communication or video visits are offered either scheduled or on-demand. Based on the outcome of the telehealth visit, no testing may be recommended. In this case, EDs may recommend continuing self-monitoring, social distancing, and provide clear follow up directions. Alternatively, one of several other options are recommended as described. *See Appendix 2
Staffing Model: In the BJC model nurses are most commonly utilized in the initial phases of screening with APPs and physicians making final tele-triage decision. Based on lessons learned from BJC, we also recommend using several different types of staff in sites considering a similar program. These include medical assistants for registration, social workers and medical students for follow-up to communicate test results, and paramedics for home testing and follow up. Forward triage via telehealth is also ideal for older clinicians including nurses, advanced practice providers, and physicians, who are more susceptible to COVID-19. They can protect themselves by virtually screening patients and help decompress overcrowded EDs.12
Summary
Facility needs and needs of the patients it serves should be the priority for establishing any telehealth program. Since the ability to conduct a telehealth visit is already available in most smart phones, tablets, and computers, the focus should be on the workflow in any telehealth program within an ED. In the case of nursing homes, the most common approach is a provider-to-provider model where EDs provide consultation to nursing home providers. For rural and critical access hospitals, partnering with an organization with an existing telehealth platform will ensure timely access to specialists for complex patients. Finally, when implementing telehealth for forward triage in primary care and ED’s, prioritizing which patients can be seen virtually and, if needed in-person is key. Considering most parts of the country are under variations of shelter in place mandates, the ability to virtually connect with patients while reducing use of personal protective equipment (PPE) and exposure to ED providers, positions telehealth as a critical tool during this pandemic.
Table 2
Top Ten Telehealth Tips for Clinicians
- Prior to launching your program, make sure you know your institutions policy on what is and is not an appropriate telehealth visit. For example, complaints of chest pain and loss of neurologic function may mandate onsite evaluation.
- Make sure the patient is registered and you have a way to document the encounter, ideally using your normal electronic health record.
- Secure a private setting and ensure adequate audio and/or video connectivity.
- Prior to a visit try and understand the reason for visit and past medical history. If a scheduled visit, have the requesting site send along any relevant details about the patient prior to consultation.
- Introduce yourself at the start of the visit, including name and role.
- Set expectations:
- let the patient know what to expect from the visit, including limits of telehealth and benefits.
- make sure the patient can see/hear you.
- ask the patient if this is their first telehealth visit.
- integrate the tele-presenter during the visit and into the conversation.
- On camera tips:
- Focus on the camera rather than the screen as this allows for pseudo-eye contact.
- Use positive body language: nod your head to acknowledge understanding, maintain an open chest and lean forward, avoid lots of hand motions that can be distracting, especially if the connection is not ideal.
- Switch from a telehealth visit to an in-person visit if a more detailed physical exam is required and/or:
- escalates to an emergent situation
- requires specialist consultation
- Before ending a visit:
- reiterate next steps.
- review treatment plan.
- leave time for questions.
- After a visit:
- document the visit using your standard documentation tool.
- contact the patient’s primary care provider if possible.
Box 2
Patient Scenario Follow-Up
A 25-bed community-based Emergency Department (ED) is located 100 miles from the nearest academic medical center. The community-based ED is the only ED within a 50-mile radius and serves a local rural population as well as 15 nursing homes in the area. The ED Medical Director is concerned that her already understaffed ED will be overwhelmed in the coming weeks with an anticipated surge in visits from COVID-19. She is aware that telehealth may be an important tool in triaging and treating patients, and in general is currently reimbursable.
Q1: What telehealth protocols and programs should be implemented to reduce overcrowding?
A: A forward triage protocol and training program for nursing homes to connect with an established telehealth hub to optimize transfer decisions and have access to geriatric and specialist expertise.
Q2: How can she incorporate forward triage across a variety of settings?
A: Identify staffing and clinical needs at the local site and implement a protocol designed to address the needs of providers “on the ground”. For example, nurse triage or provider-to-provider.
Q3: How can ED’s address the needs of the community while protecting their own staff?
A: Leverage a nurse triage to help identify priority patients and use staff not currently in the ED, during administrative time, or providers who may be more at risk for infection to facilitate telehealth visits, this will also preserve personal protective equipment (PPE) for in-person ED visits.
Q4: Given limited resources and time, what options does the Medical Director have?
A: Partner with a facility that already has an established telehealth program, and if her ED is providing telehealth services, work with her billing team to ensure ED services delivered via telehealth are billable under modifier 95.
Q5: What guidance can the Medical Director provide in helping her clinicians be ready to provide care via telehealth?
A: Develop a “tip sheet” with the following: Review reason for consult before the telehealth visit, set expectations before you begin your assessment, review the treatment plan together before ending a visit and leave time for questions.
Acknowledgements
Co-Editors in Chief: Michael L. Malone, MD and Teresita M. Hogan, MD, FACEP
Conflict of Interest: Michael L. Malone owns stock in Abbott Labs and Abbvie.
The authors would like to thank West Health, The John A. Hartford Foundation, and the Institute for Healthcare Improvement for their contributions and collaboration in creating this edition of JGEM. Finally, the authors thank Stephanie Steger for her administrative support.
Affiliations
Kelly Ko, PhD: West Health Institute
Michael Kurliand, MS, BSN, RN: West Health Institute
Kevin Curtis, MD, MS: Dartmouth-Hitchcock Health
Christopher Palmer, MD: Washington University
Michelle Naimer, MD, MHSc: Sinai Health
Scott Rodi, MD, MPH: Dartmouth-Hitchcock Health
Zia Agha, MD, MS: West Health Institute
References
- Technology for Telehealth. American College of Physicians website. https://www.acponline.org/practice-resources/business-resources/health-information- technology/telehealth/technology-for-telehealth. Accessed April 20, 2020.
- Cyr ME, Etchin AG, Guthrie BJ, Benneyan JC. Access to specialty healthcare in urban versus rural US populations: a systematic literature review. BMC Health Serv Res. 2019;19(1):974. Published 2019 Dec 18. doi:10.1186/s12913-019-4815-5
- Krushinskie A. COVID-19 Insurance Policy Changes. American College of Emergency Physicians website. https://www.acep.org/corona/COVID-19/covid-19-articles/covid-19-insurance-policy-changes/. March 30, 2020. Accessed April 20, 2020.
- McMichael TM, Currie DW, Clark S, et al. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington [published online ahead of print, 2020 Mar 27]. N Engl J Med. 2020;NEJMoa2005412. doi:10.1056/NEJMoa2005412
- Grabowski DC, Joynt Maddox KE. Postacute Care Preparedness for COVID-19: Thinking Ahead. JAMA. Published online March 25, 2020. doi:10.1001/jama.2020.4686
- COVID-19 Resource Center. West Health website. westhealth.org/covid-19-resource-center/. Accessed April 22, 2020.
- About Rural Health Care. National Rural Health Association website. ruralhealthweb.org/about-nrha/about-rural-health-care. Accessed April 23, 2020.
- Healthy People 2020. Office of Disease Prevention and Health Promotion website. healthypeople.gov/2020/topics-objectives/topic/older-adults. Accessed April 23, 2020.
- Rural Aging. Rural Health Information Hub website. ruralhealthinfo.org/topics/aging. Accessed April 20, 2020.
- Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
- Lemoyne SE, Herbots HH, De Blick D, Remmen R, Monsieurs KG, Van Bogaert P. Appropriateness of transferring nursing home residents to emergency departments: a systematic review. BMC Geriatr. 2019;19(1):17. Published 2019 Jan 21. doi:10.1186/s12877-019-1028-z
- Buerhaus PI, Auerbach DI, Staiger DO. Older Clinicians and the Surge in Novel Coronavirus Disease 2019 (COVID-19). JAMA. 2020 (in press).
Disclaimer
The situation with COVID-19 is changing rapidly and many national and state websites are providing daily or more frequent updates. Please check those websites daily for any updated information and check the date that the website was most recently revised.
The content provided above is current as of 5-11-2020.
For our full disclaimer please see this link.
Appendix 1
SAN DIEGO COUNTY SENIOR EMERGENCY CARE INITIATIVE WORKFLOW
Appendix 2
FORWARD TRIAGE PROTOCOL: BARNES JEWISH CHRISTIAN HEALTH SYSTEM & WASHINGTON UNIVERSITY IN ST. LOUIS