Two-Step Approach to Delirium Screening
The number of formal delirium assessments needed can be reduced.
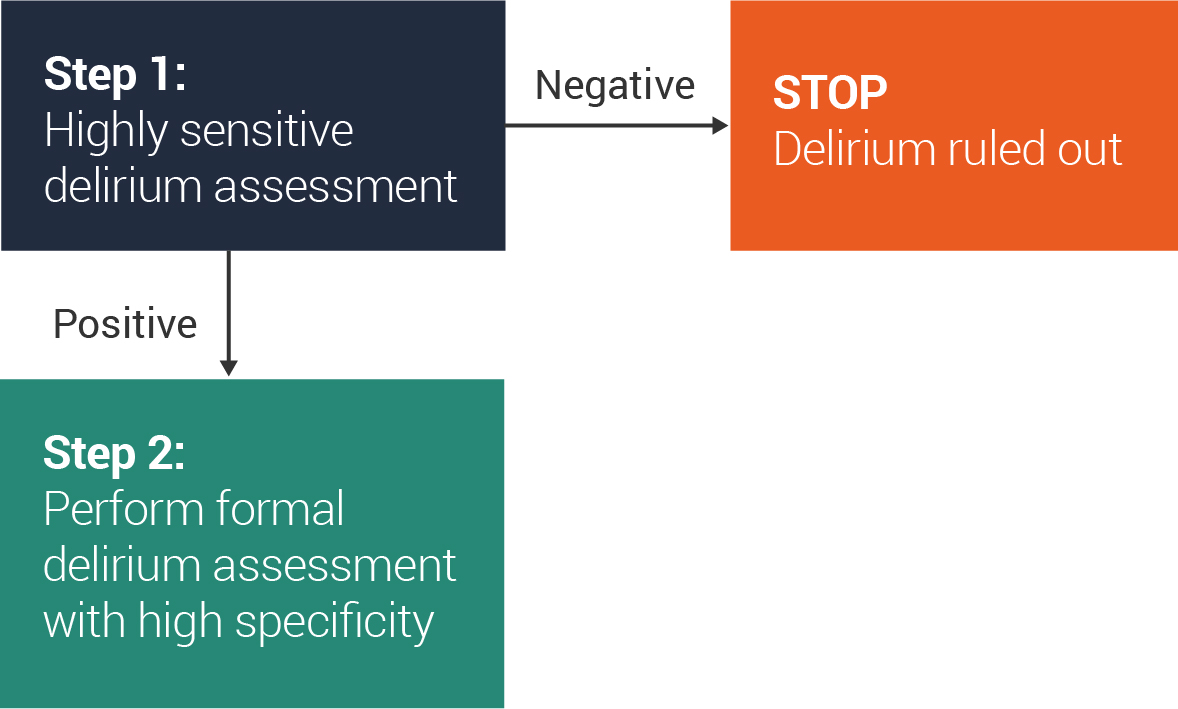
Another approach to improving delirium detection in the ED is to use a 2-step approach to delirium screening.
Step 1
The first step would be to perform a very brief (<20 seconds) delirium assessment that is highly sensitive for delirium to rapidly rule out delirium. This could be performed as part of the initial nursing or triage assessment. Ideally, the highly sensitive delirium screen should have a sensitivity >90% and specificity >50%.
Delirium Triage Screen (DTS)
The DTS fulfills these criteria (98% sensitive; 55% specific) and has been validated in older ED patients. Additional details are provided in the next slide. Fick et al observed that using the combination of months of the year backwards and asking “What is the day of the week?” was 93% sensitive and 64% specific for delirium in older hospitalized patients.
-
- A negative step 1 screen would rule out delirium and no additional delirium assessment is needed.
- A positive step 1 screen would trigger a formal and highly specific delirium assessment at the patient’s bedside to rule in delirium.
Step 2
For the second step of this screening approach, the CAM, bCAM, CAM-ICU, 3D-CAM, or 4AT are examples of more specific delirium assessments that can be used.
This screen could be performed by a trained bedside nurse or treating physician experienced in performing delirium assessments.
NOTE
The overall diagnostic accuracy of this 2-step approach to delirium screening will largely be limited by the sensitivity and specificity of the delirium assessment in the second step. We provide an example of this on the next slide.
References
Han JH, et al. Ann Emerg Med. 2013;62(5):457–465
Fick DM, et al. J Hosp Med. 2015;10(10):645–650
Abbreviations
3D-CAM, 3-Minute Diagnostic Interview for CAM
4AT, test for delirium & cognitive impairment (Alertness, Age-birthdate-place-current-year, Attention, Acute change)
bCAM, brief CAM
CAM, Confusion Assessment Method
CAM-ICU, CAM for the Intensive Care Unit
DTS, Delirium Triage Screen
ED, emergency department