Introduction
The agitated older patient presents a particularly difficult blending of the emergency principles of stabilization, diagnosis, and treatment. This happens because rapid behavioral control might obscure or delay diagnosis, and the treatment of agitation could allow worsening of the underlying causative disorder(s). However, urgent behavior control may be required in older patients seen as a danger to themselves or overwhelming the capacity of the emergency department (ED) staff. Physicians are asked for immediate problem resolution, nurses need to ensure patient safety, and both must maintain continued responsiveness to all the patients in their care. “Can you give me something to calm down the patient in room 16?” The implication is to fix the problem now. However, the optimal management path follows five core principles in order:
-
- Assess
- Diagnose
- Evaluate
- Prevent
- Treat
The American College of Emergency Physicians developed the “ADEPT Tool” for management of confusion and agitation in the older ED Patient. The ADEPT Tool highlights the need to first recognize the myriad and often multifactorial causes of behavioral changes in older adults, including those in the ED environment. Then the final step may involve specific pharmacologic management.1
The charge for emergency providers is to facilitate assessment and treatment of the underlying condition(s) while ensuring a safe environment for patients and staff. “Assess” includes evaluation of life-threatening and immediately treatable conditions of hypoxia, hypoglycemia, acute MI, cerebral ischemia, hypotension, and sepsis. Pain commonly causes agitation and must be identified and treated, ideally with non-sedating non-opioid medications.
Establishment of baseline mental status and rapidity of change are essential, but require contact with family, caregivers, or facilities that may not be readily available.
The most common causes of acute alterations in mental status in older persons are infection, neurologic disorder, metabolic or electrolyte disorder, medication effect, and deterioration of underlying medical conditions including the behavioral and psychiatric symptoms of dementia. Commonly multiple factors are responsible; hence assessment does not stop at the first factor identified (see Table 1). Systematic evaluation and treatment for all contributing conditions must continue until full evaluation is complete. ED staff must understand that the hectic ED environment often contributes to agitation and strive to diminish the impact of this familiar iatrogenic cause.
Agitation and hyperactive delirium are commonly seen in persons with dementia.2 and increase with severity of cognitive decline.3 However, emergency providers only establish this diagnosis in fewer than 20% of newly delirious patients.4,5 The presence of new hallucinations points to delirium and, with exception of Lewy body dementia, hallucinations are rarely seen in dementia. Adverse medication effect causes delirium in from 12-39% of cases.6 The patient’s evaluation must include physical examination for signs of potential non-accidental trauma or neglect- important to consider in people with dementia or frailty.
Nursing is typically the front line of behavioral management and it occurs in real time at the bedside. It is the nurse who implements most non-pharmacologic strategies and sets the emotional tone in patient interactions. Nurses control toileting, hydration, nutrition, and ambulation. They are in optimal position to manage the patient’s environment,9 and to varying degrees nurses are able to affect the interaction with caregivers/family/visitors. Nurses are the first to note pain and success or failure in its management. Similarly, nurses can set the timeline of “tolerance” for agitated behavior and determine its periodic reevaluation. Prevention and early identification of patients at risk for delirium, falls, and behavioral issues are effective strategies for patient safety.10
Nurses can help manage therapeutic interventions and minimize distractions because preventing excessive stimuli limits agitation. This can be accomplished by closing the door to the patient’s room (if possible, in certain ED settings), having as few people present as possible during procedures, being organized and completing every intervention in a calm and efficient manner, and speaking softly in simple language throughout every exchange.11
Table 1
Emergency Department Care Strategy for Agitated Elder Patients
- Always approach agitated patients with compassion and empathy. A calm attitude sets the tone for optimal encounters, ideal staff leadership, and successful outcomes.
- Identify the underlying cause(s). Multiple causes are the rule. The more factors that can be addressed the higher the chance of successful treatment.
- Prevent worsening symptoms – both of the underlying cause(s) and of the agitated behavior.
- Remember family and caregivers. Offer support, educate, and enlist assistance of these individuals as appropriate. A caring person at the bedside decreases patient agitation, empowers the caregiver, and eases staff burden. ED volunteers may sometimes be used to assist in these cases,7 and the most cost effective sitter role appears to be use of a trained volunteer.8
- Recognize that all agents for treatment of acute agitation carry potential for significant adverse events.
- Avoid over sedation which may both delay optimal diagnosis and lead to iatrogenic and avoidable poor outcomes.
Non-Pharmacologic Strategies
Aggression, exit-seeking, and resistance to care, may be considered a response to unmet needs in older adults with dementia and/or delirium. These basics should always be implemented prior to seeking medications.
- Always begin with a calm demeanor, verbal de-escalation, distraction, and reassurance.
- Meet the patient’s needs for frequent reorientation, hydration, nutrition, toileting, pain and nausea management, and treatment of underlying conditions.
- Ensure the patient’s hearing and visual impairments are addressed as part of establishing essential communication.
- Remove triggers of loud noises and other noxious stimuli wherever possible. Alarms, glare, and background distraction (such as the television) are frequent ED triggers for agitation and anxiety. Limitation of Tethers is important. IVs, Foley catheters, pulse oximetry, and blood pressure cuffs can frustrate and irritate vulnerable older adults. Lighting should be kept free of shadows and glares with low lighting restricted to sleep time.
- Recognize the ED is a “deliriogenic environment” which by its very nature causes anxiety and agitation, especially with ED length of stay ≥10 hours.12 Environmental modifications can be helpful and include: reorientation or calming strategies such as involvement of family members or volunteers, use of sitters, movement to position of best observation, falls and injury prevention, limitation of tethers, one to one nursing, hydration, nutrition, and enhancing mobility by routinely (on a regular schedule) ambulating the patient who has a prolonged ED stay. Routine toileting every 1-2 hours can be incorporated into this ambulation strategy. Soft music and singing have been noted to decrease agitation in dementia.13,14,15
Pharmacologic Options
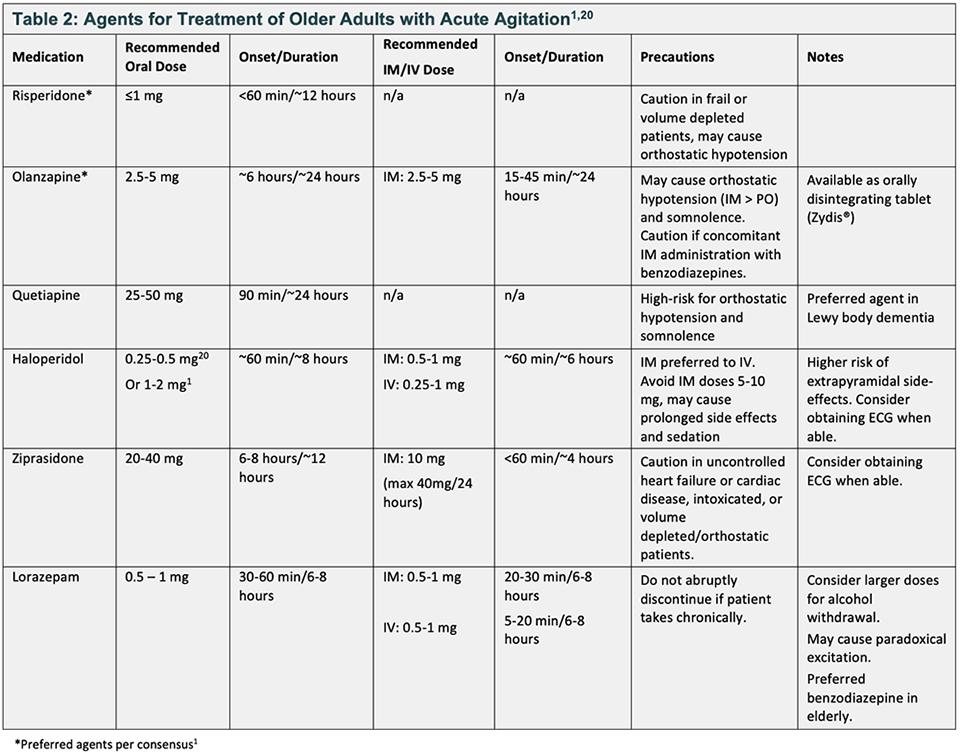
The goal of pharmacologic treatment of agitation is to calm the patient so that he or she may be accurately and safely assessed, and their underlying condition(s) treated. The ideal agent will calm the patient so they can contribute to their own care and will not interfere with disposition due to over sedation. All of the medications discussed in Table 2 below are listed as potentially inappropriate by the Beers criteria.16 These medications may contribute to prolonged sedation or paradoxical agitation. Treatment should be initiated with oral medications when possible, utilizing a “start-low, go-slow” dosing scheme. Remember that repeat doses can be administered if necessary.
When selecting pharmacologic treatment consider the impact of comorbid conditions, past response, and current medications. Older patients are sensitive to side effects and medication interactions and are more prone to polypharmacy.17 Head to head trial
data comparing agents is limited. However, best current consensus evidence prefers risperidone or low-dose olanzapine for treatment of agitation.1,17 If the patient is prescribed an antipsychotic at home, start with this medication and dose (if available in your ED).18 Antipsychotics should be used cautiously in patients with a known diagnosis of dementia as they have been associated with increased mortality in this population.1 However, this antipsychotic use mortality data was found in long term use, not one-time ED use. When considering adjunct therapies, diphenhydramine
should be avoided unless treating an acute allergic reaction or anaphylaxis, and there is no evidence that anticonvulsants treat agitation and delirium in patients with dementia.1, 17
Medication selection should be driven by the underlying cause of agitation. Anticholinergic medications (e.g. olanzapine, diphenhydramine) may exacerbate delirium. Consider risperidone or haloperidol for these patients. For patients with
Parkinsonism or suspicion for Lewy body dementia antipsychotics especially haloperidol should be avoided.
If patient care requires treatment with an antipsychotic, quetiapine is the preferred agent.18 When treating primary psychosis consider atypical antipsychotics ± benzodiazepines. Alcohol or benzodiazepine withdrawal should be treated with lorazepam ± thiamine, while haloperidol is the preferred agent in patients with acute alcohol intoxication.19
Conclusion
In summary, agitation can be a symptom of serious underlying conditions in older adults and is often multifactorial. Optimal management begins with a calm understanding approach and a systematic assessment with attention to each problem (Table 3). Eliminate deliriogenic ED triggers, address unmet needs and pain, and treat underlying conditions. Pharmacologic management when needed should be oral, “start-low go-slow.” Preferred agents are risperidone and olanzapine.
Table 3:
Five Key Take Home Points
- Remember the optimal treatment path for older adults with agitation is ADEPT →
Assess-Diagnose-Evaluate-Prevent-Treat
- Identify the underlying cause(s). Multiple factors are common. Prioritize but address them all.
- Ensure physical needs are met, optimize patient comfort, and decrease the “deleriogenic” factors in the hectic ED environment.
- Drug treatment principles: use oral agents if possible, “start-low go-slow.”
- Risperidone or low-dose olanzapine are preferred agents.
Acknowledgements
Co-Editors in Chief: Michael L. Malone, MD and Teresita M. Hogan, MD, FACEP
Conflict of Interest: Michael L. Malone owns stock in Abbott Labs and Abbvie. The authors and editors have declared no conflicts of interest for this article.
References
- Shenvi C, Kennedy M, Austin CA, Wilson MP, Gerardi M, Schneider S. Managing Delirium and Agitation in the Older Emergency Department Patient: The ADEPT Tool. Ann Emerg Med. 2020 Feb; 75(2):136-145. doi: 10.1016/j.annemergmed.2019.07.023. Epub 2019 Sep 26.https://www.acep.org/patient-care/adept/
- H. Han, S. Eden, A. Shintani, et al.Delirium in older emergency department patients is an independent predictor of hospital length of stay. Acad Emerg Med. 2011; 18:451-457.
- Siafarikas, G. Selbaek, T. Fladby, et al.Frequency and subgroups of neuropsychiatric symptoms in mild cognitive impairment and different stages of dementia in Alzheimer’s disease. Int Psychogeriatr. 2018; 30:103-113.
- M. Hustey, S.W. MeldonThe prevalence and documentation of impaired mental status in elderly emergency department patients. Ann Emerg Med. 2002; 39: 248-253
- A. LaMantia, F.C. Messina, C.D. Hobgood, et al. Screening for delirium in the emergency department: a systematic review. Ann Emerg Med. 2014;63: 551-560.e2
- Alagiakrishnan, C.A. Wiens. An approach to drug induced delirium in the elderly. Postgrad Med J. 2004; 80:388-393
- Sanon M, Baumlin KM, Kaplan SS, Grudzen CR. Care and Respect for Elders in Emergencies program: a preliminary report of a volunteer approach to enhance care in the emergency department. J Am Geriatr Soc. 2014; 62(2):365-70. doi: 10.1111/jgs.12646. Epub 2014 Jan 15.
- Carr FM, The role of sitters in delirium: An update. Can Geriatr J. 2013; 16(1): 22-36.
- Somes J, StephensDonatelli N, Kuhn S. Controlling Aggressive Behavior in the Geriatric Patient Journal of Emergency Nursing. 2011;37(3):275-277.
- Laws D, Crawford CL. Alternative strategies to constant patient observation and sitters. The Journal of Nursing Administration. 2013; 43(10):497–501. DOI: 10.1097/NNA.0b013e3182a3e83e
- McCloskey RM. Caring for patients with dementia in an acute care environment. Geriatric Nursing. 2004 May-June; 25(3): 139-44.
- Bo, M. Bonetto, G. Bottignole, et al. Length of stay in the emergency department and occurrence of delirium in older medical patients. J Am Geriatr Soc. 2016; 64: 1114-1119.
- Ragneskog H, Kihlgren M. Music and other strategies to improve the care of agitated patients with dementia. Scand J Caring Sci. 1997; 11:176-182.
- Clark A, Lipe A, Bilbrey M. Use of music to decrease aggressive behaviors in people with dementia. J Gerontol Nurs. 1998; 24:10-17.
- Devere R. Music and Dementia: An Overview. Practical Neurology June 2017. Available at https://www.verywellhealth.com/using-music-in-alzheimers-disease-97624.
- American Geriatrics Society 2019 Updated AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc; 2019; 00:1-21. DOI: 10.11111/jgs.15767 https://qioprogram.org/sites/default/files/2019BeersCriteria_JAGS.pdf
- Aftab A, Shah AA. Behavioral Emergencies Special Considerations in the Geriatric Psychiatric Patient. Psychiatr Clin N Am. 2017; 40:449-62.
- Kurlan R, Cummings J, Raman R, Thal L, et al. Quetiapine for agitation or psychosis in patients with dementia and parkinsonism. Neurology. 2007; 68(17):1356–1363. doi: 10.1212/01.wnl.0000260060.60870.89
- Bessey LJ, Radue RM, Chapman EN, et.al. Behavioral Health Needs of Older Adults in the Emergency Department. Clin Geriatr Med. 2018; 34(3):469-89.
- Wolters Kluwer Clinical Drug Information, Inc. (Lexi-Drugs). Wolters Kluwer Clinical Drug Information, Inc.; February 18, 2020.
- Capezuti E. Minimizing the use of restrictive devices in dementia patients at risk of falling. Nurs Clin North Am 2004; 39: 625–47.
- Mion L. Establishing alternatives to physical restraint in the acute care setting: a conceptual framework to assist nurses’ decision making. AACN Clinical Issues; 1996; 17:592-602.